
Piriformis syndrome
A glute cause analysis, Part 1

Thanks for reading the 22nd edition of my sciatica newsletter. This newsletter tracks my research as I write a book about lumbar radicular pain!
If you want to start a fight in a bar full of physios, mention piriformis syndrome.
Judging by the number of people I meet who tell me they have it, there are some clinicians out there diagnosing it every week. But some will tell you it doesn't even exist. What's going on?
First, a word on terminology. Like Father Christmas, who is increasingly now called 'Santa Claus', piriformis syndrome is now often goes by another name. This is because the piriformis is only really one of many structures in the deep gluteal space that could entrap or irritate the sciatic nerve. There are also the gluteal muscles, vascular abnormalities, space occupying lesions, fibrous bands, and all those little hip muscles. So we are now to recognise piriformis syndrome as a sub-type of a broader condition called "deep gluteal syndrome".

Deep gluteal syndrome was coined a couple of decades ago, but has only really become common parlance in the last five years or so. It's defined as "a non-discogenic sciatic nerve disorder with entrapment in the gluteal space".

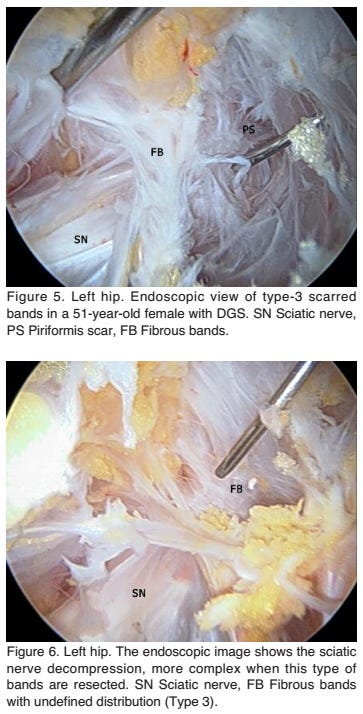
(In case you are wondering, here are some of the "fibrous bands" that could entrap the sciatic nerve:)

So what does deep gluteal syndrome look like?
We are told it looks like this:
Buttock pain
Tenderness on deep palpation of the buttock
Aggravation of pain on prolonged sitting
Passive stretching or resisted contraction tests
So, like nerve root pain then?
Nerve root pain often looks like what people think piriformis syndrome looks like.
Let’s look at what happens in the shoulder first. Scapular pain and shoulder pain can come from the nerve root. In one study, about half of all people with cervical radiculopathy had some pain in their shoulder girdle. In another study, 20% of people with cervical radiculopathy had pain that was only in their shoulder girdle, nowhere else. To labour the point, one further study found that a good 4% of people who were referred to a specialist shoulder surgeon turned out to have cervical nerve root pain.

I might be wrong, but I don't think this will be surprising to anyone. People are quite comfortable with the idea that shoulder pain can come from the neck. Especially when it radiates down the arm and is "nervey". And even when the neck doesn't hurt. We don't have "deep shoulder girdle syndrome". Sure, there's thoracic outlet syndrome, but - again, this is just my impression - most people consider that to be a vanishingly rare condition.
So I am not sure why, when a patient has buttock pain, we go to piriformis syndrome or deep gluteal syndrome. To me, the nerve roots seem like the more likely culprit. Especially when the the buttock pain radiates down the leg and is "nervey". And even if the low back doesn't hurt.
Let me give a few examples to show that buttock pain, even isolated buttock pain, can come from the nerve root and its dural sleeve. Here's a few excerpts from the Smyth and Wright study I cite so often, where the authors tied nylon strings around patients' nerve roots during an operation, pulled on them, and recorded the sensations caused:
"[On pulling on the nerve root] the effect was immediate. The patient jumped and exclaimed that a severe pain shot into the right buttock... at the second attempt the thread was very slowly drawn upon until the patient could feel pain. This time it was not so intense: the thread could be barely touching the root. Then tension was increased and as it mounted severe pain spread from the center of the right buttock down the center of the back of the right thigh, veered laterally to the region of the biceps tendon, skipped the side of the knee, and was felt intensely on the lateral side of the calf. It ended about three inches above the lateral malleolus”
“On pulling the dural thread, an ache was felt at the medial and inferior aspect of the left buttock just at the fold. It was localized to an area about one inch in diameter and was of a mild nature.”
“On the tenth postoperative day when traction was exerted on the nerve root the only effect was an ache in the region of the wound. There was no suggestion of sciatica. On prolonging the pull for a quarter of a minute, a subjective sensation of numbness was produced in the lower lateral portion of the buttock of the left side."
In another similar study, Kuslich found it more difficult to reproduce buttock pain, but reported that it was caused "by the application of pressure on the nerve root and outer annulus simultaneously". Presumably this is a common pattern of nociception caused by a disc herniation.
One interesting recent study found that of 286 patients with a disc herniation, 168 had buttock pain. The authors also noted that almost all of those 168 had a herniation at L4/5, so perhaps that is the level that most frequently refers pain to the buttock.
Clearly, nerve root pain can be felt in the buttock. So I am really not convinced that someone having buttock pain shifts the needle that much to the primary problem actually being in the buttock!
What about tenderness?
What about the second clinical feature of deep gluteal syndrome, "tenderness on deep palpation of the buttock"? Well, this too has long been a recognised symptom of nerve root pain. In 1943, O'Connell wrote that "in many cases [of herniation-induced nerve root pain] tenderness along the course of the sciatic nerve is present. It is frequently most severe over some area such as the buttock, the lower third of the back of the thigh, or the calf..." In 1948, Falconer made a similar observation, writing that "in a few of our cases of [nerve root pain] tender spots which could be described as "nodules" were observed in the muscles of the buttock and calf... we always found an associated disc prolapse." A more recent study attempted to quantify this phenomenon, and found that 71% of 271 patients diagnosed with radicular pain had sore spots in their bums, compared to only 2% of control volunteers. There have even been attempts to use buttock tenderness as a 'special test' for radicular pain.
I am not going to get into the debate about what causes these sore spots (you will be relieved to hear!) Suffice to say that local tenderness does not mean a local primary cause.
Let's briefly tick off the last two features of deep gluteal syndrome. The third feature is the aggravation of pain on prolonged sitting. I don't think I will have to work too hard to convince anyone this is also a common feature of nerve root pain, or any spinal pain! And the last feature is "passive stretching or resisted contraction tests". Passive stretching tests, whether of the piriformis or the nerve itself, test nerve sensitivity to movement, which is a feature of nerve root pain. Assuming resisted contraction tests of the piriformis muscle actually contract the piriformis muscle and squeeze the sciatic nerve, this too could easily be painful for people with nerve root pain. It's just another neural mechanosensitivity test.
But an injection helped!
One thing you often hear is that clinicians inject people with deep gluteal syndrome in the deep gluteal space and they get better. I saw an emergency department doctor on twitter saying he does this for patients who come in with acute neuropathic leg pain. His point was that this proves piriformis syndrome is underdiagnosed because most of his patients who other doctors would have diagnosed with radicular pain got better with a gluteal injection.
I am all for pain relief and think it is under-used for people with acute neuropathic pain. So I fully support this doc! But I think his conclusion that his patients had piriformis syndrome is wrong. Kibler and Nathan recognised in 1960 the thoroughly weird phenomenon that if someone has a nerve injury you can inject anaesthetic distal to the injury site and they will get pain relief. The effect can even outlasts the duration of the anaesthesia. A more recent study by North and colleagues found the same thing. They wrote, "In the great majority of our patients, known to have radiculopathy, we have found that sciatica is relieved by temporary local anesthetic blocks distal or collateral to any putative anatomic source of pain". In fact, O'Connel, who I quoted above observing that people with nerve root pain often have sore spots in their glutes, also observed that they feel better when you inject them, but only for a short time. Anything I say about why distal nerve blocks relieve proximal nerve pain would be speculation. But they do!
So the supposed common features of deep gluteal syndrome - buttock pain, buttock tenderness, pain on sitting and neural mechanosensitivity - are all, in fact, to greater and lesser extents, classic signs of nerve root pain.
🎅 Why piriformis syndrome is like Santa Claus…
Looking at what I've written, it looks like I've set out to do a hatchet job on piriformis syndrome/deep gluteal syndrome. That's not really where I'm going! In part 2 and, if I really ramble, part 3, we are going to look at what deep gluteal syndrome "should" look like, given what we know about compressive neuropathies, and look at the most persuasive evidence that it does exist.
And I think it does exist! I just think it's really rare. The way I see it, piriformis syndrome is like Santa. Santa exists, but you hardly ever see the real Santa. If you think you have, it's probably just some bloke dressed up to look like him. Piriformis syndrome exists too. But you hardly ever see that, either. And if you think you have, it's probably just some boring old nerve root pain in disguise…
As always, I'd love to hear your thoughts, particularly if you think I've missed something, or if you disagree (unless you disagree that Santa is real.)
🎄 Bits and baubles 🎄
Sorry for not linking to google drive files of all the papers this week. It’s a bit time consuming and I have to buy a turkey now! Please do not hesitate to email if you have difficulty accessing anything.
Last week I mentioned nervously that I was going to see if I could format an ebook in Adobe InDesign. It took a while to figure it out but once I had, it’s not too difficult. Here’s what it looks like (the text isn’t the book, it’s just last week’s newsletter)




You might remember that I was wondering a couple of months ago about putting the book out in three installments, to try to keep me going psychologically. I abandoned the idea for various reasons (thanks to some people who gave me positive and negative feedback on it). But after talking to some friends (thanks Nils and Sagar) I have decided to put the book out in two parts. This is because, although the rough manuscript is pretty much done, to redraft, edit, illustrate, format and produce the whole thing to the standard I want will take many weeks. So rather than compromise it for the deadline or drag the project to who knows when, I will split the work into two. My self-imposed deadline is still February 1st, but it is for part 1 of 2!
That’s it for this week. Happy Christmas! I wish you all peace and good will.
Tom
Very detailed. Would relaxing the piriformis muscle with a glute massager help?
When is the lumbar radiculopathy book going to be ready?