
Recovering from radiculopathy
How long do motor and sensory deficits take to recover?

Thanks for reading the 12th edition of my sciatica newsletter. This newsletter tracks my research into all things lumbar radicular pain!
This week’s podcast was a sciatica story with Drew Jordan. I found Drew through his epic, incredibly generous one-an-a-half-hour video on how he manages his sciatica. It was really interesting to hear how he worked out his pain triggers and his insightful “big picture” perspective on pain. You can listen here.
This week I want to answer an interesting question from a reader who has a recent onset of radiculopathy:
"I wonder how long the motor and sensory deficits take to recover - is there a difference for both? I imagine it can depend on the level of compression of the disc"
I didn’t know the answer at first but after a bit of reading, here’s what I’ve come up with…
Loss of function
First off: this is a question about “loss of function”. Apparently, I caused a bit of confusion when I mentioned this in my TherapyLive talk. But loss of function is just what we are testing for in the classic “neuro exam”: loss of muscle power, loss of sensation, and loss of reflex.
People with radiculopathy have loss of motor and sensory function because conduction is impaired somewhere in the nervous system, presumably the nerve root.
Incidentally, people with radiculopathy rarely have total motor loss because the motor fibers from each root will mix up in the peripheral nervous system so that any one nerve trunk contains fibers from a few different roots. This is why you can sit on your leg, compress the nerve trunk and have your foot go totally dead after a few minutes, but very few people with radiculopathy have a total foot drop.
People with radiculopathy also rarely have total sensory loss because dermatomes overlap a good deal.
Nevertheless, these "loss of function" signs are an important part of the clinical picture for people with radiculopathy.
Compression causes loss of function
The reader who submitted this question is right that the more compressed a nerve root is, the greater the loss of function. (Something I love about radiculopathy: sometimes structure actually matches up to clinical presentation!) This is because compression reduces blood flow to the neurons. Without blood, the neurons don't have the oxygen and nutrients they need to function. This blood flow backup also causes oedema, which further impairs conduction. The more compression, the less blood flow; the less blood flow, the greater the potential conduction block and nerve damage.
And indeed, large, uncontained extrusions and sequestrations are more associated with loss of function than smaller, contained herniations.
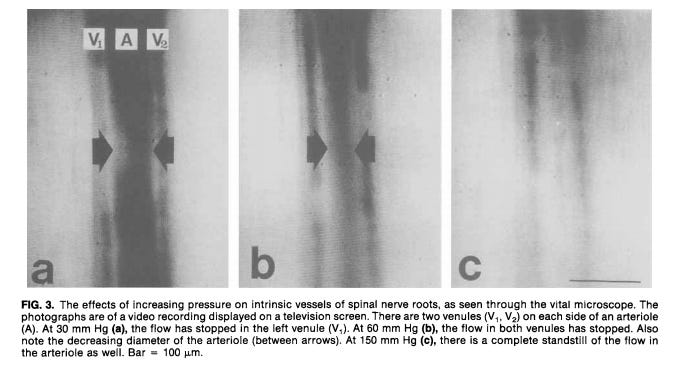
Decreasing blood flow with increasing constriction in a pig’s nerve root. From Ollmarker et al (1989).

From Lin et al. (2014)
Of course, it's not all about compression! Studies in dogs and rabbits have shown contact alone from the nucleus pulposus - an irritant to nerves - can cause loss of function.
How many people with radiculopathy recover their nerve function?
Most studies look at motor, not sensory function.
A review by Balaji et al. (2014) found that 38% of patients completely recovered motor function and 50% made a recovery to at least a power grade 4. These figures do include both surgical and non-surgical patients, but the difference between the two groups was very slight.
Unfortunately, the wide range of results amongst quite a small number of studies included in the review makes it quite hard to take these figures as gospel. I think they are slightly skewed to the low side because in some of the included studies all patients had profound weakness, which doesn’t represent the typical radiculopathy caseload for rehab clinicians.
How quick is recovery?
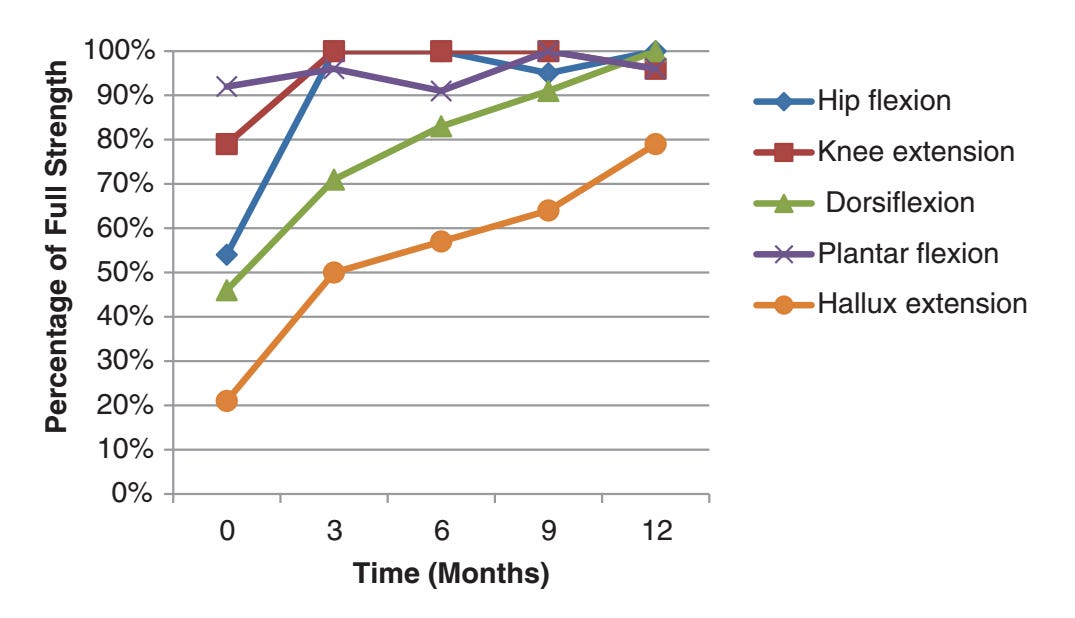
If we look closer at some individual studies we can get an idea of how long it takes. This nice graph from Akuthota et al. shows that people recovered dorsiflexion and big toe extension (green and orange lines) most quickly in the first three months and gradually but steadily thereafter.
This analysis by Overdevest et al. is useful because it included patients with acute onset of symptoms. The green bars are people who had surgery, the blue conservative treatment. People who didn't have surgery recovered their muscle strength slowly but surely over the course of a year.

There is a similar story from trial by Butterman. The black bars, representing people who were treated with an epidural injection, show that most people recovered function between three and six months with others joining them gradually over three years.

Finally, Grøvle et al. also found that people's subjective sense of weakness recovered most quickly in the first three months and very gradually thereafter.

Of course, in all these studies there are a substantial minority of patients who have not recovered full muscle power after a year or more.
What about sensation?
Sensation is less studied. But in the limited data we have, sensation does not seem to recover as well as muscle power. Suri et al. found that after one year, 62% of patients with motor loss had recovered but just 47% had recovered from their sensory loss, rising only slightly to 53% after two years. Baluegue et al. found something similar.
I think I need to look for more studies on this. I wouldn’t think much of it, but it fits with basic science that shows sensory axons are more vulnerable to ischaemia than motor axons. Pedowitz et al. seemed to confirm this goes for nerve roots too, in their studies using pigs.
So, it seems that
On the whole, large, uncontained herniations cause more loss of function
Loss of function recovers most quickly in the first three months or so
Even after a year or more, people can still recover function
Sensation might take a bit longer to return than strength
At least 10% of people and maybe as many as 60% will not regain full function.
I’m going to work on the wide range in that last bullet point to get a better idea of how many people recover full function…
As ever, I’d love to hear your thoughts, particularly if you disagree or feel like I’ve missed something.
That’s it for this week! There is not much other news except that I finally have a desk. So this is the first edition of the newsletter in a while not to be coming to you from the floor or a fold-out camping chair. And the weather is finally becoming less unbearable in Houston, so we’re hoping to get out and see the city a bit soon.

The desk of a very happy man