


Research review!
Inflammation, bums vs backs, timing of disc regression and more...

Thanks for reading the 14th edition of my sciatica newsletter. This newsletter tracks my research into all things lumbar radicular pain!
This week's podcast was with Giacomo Carta.
Giacomo is a basic science researcher in neuromechanics, neurorepair and neuroplasticity. He’s also a physical therapist! We discussed his research and his hopes for the future of neurodynamics, nerve pain treatment and physiotherapy in general.
Research review!
This week I wanted to summarise some of the most interesting papers I’ve seen published in the last month or so.
Inflammatory signs
As I’ve mentioned before, there are a lot of possible mechanisms behind radicular pain (inflammatory, ischaemic, nociceptive, neuropathic…) but there isn't really a way to say which ones are most important or most common, much less for any one patient. If we could know, it might (might!) help us to direct treatments.
Ford et al. tried to work out a way for us to tell which patients have inflammatory type pain. They took 40 patients who underwent surgery for their lumbar disc herniations and examined the disc material for histological signs of inflammation (for example, the presence of macrophages). 11 of the 40 patients were classified as "positive" for inflammatory features. (I wish I had guessed how many before reading the results, I think I would have guessed higher). Then they examined this finding against reams of data they had collected on the participants beforehand to see if any factors "predicted" which of them would have inflammatory signs.

They found a cluster of signs that distinguished the eleven inflammatory patients.
Back pain less than 5/10 (the strongest single factor)
Pain was worse the next day after injury (does this represent the timing of the inflammatory response?)
Flexion was reduced to between 0-30 degrees
Just to complicate things, a "clinical inflammation score" of >/=3. A "clinical inflammation score" is one point for each of 1) constant symptoms; 2) morning stiffness greater than 60 minutes; 3) a short walk not easing symptoms; 4) significant night symptoms
This is a very small study and of course the results need to be tested on a second group of patients... but I am really rooting for this kind of research. I hope that in the years to come we will be able to say which treatments will benefit whom. I know there is a lot of (understandable) scepticism about that, though.
Bum vs Back
One of the biggest divides in the sciatica world, if there is such a thing, is what on earth to make of cases when someone apparently has classic radicular pain but there's nothing on their MRI to explain it. "Piriformis syndrome" (now, "deep gluteal syndrome") has been the go-to explanation for some, while others maintain that it's much more likely that the problem did originate in the spine but the disc has resorbed, or MRI is not sensitive enough. It's a debate between the "bum people" and the "back people." (And of course there’s the “brain people”…)
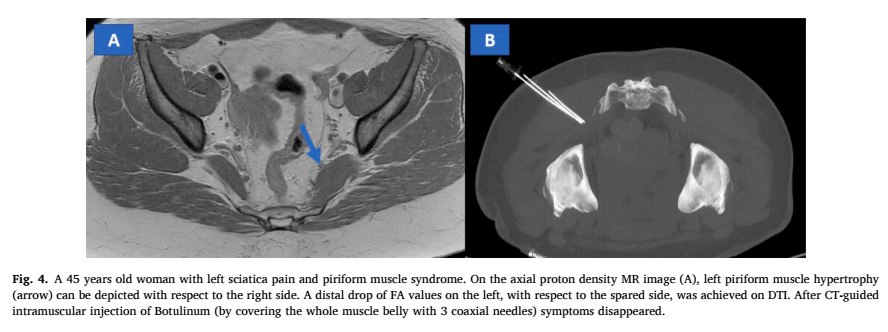
Foti et al. took 17 patients with sciatica but nothing on their spinal MRI and used diffusion tensor imaging to examine their pelvis. They found something that might explain the pain in 12 of the 17! Among them, four people had endometriosis plaques on their sciatic nerve (is that on your sciatica differential?). In a win for "deep gluteal syndrome", three had hypertrophied piriformis muscles and two had similar findings for other small muscles in the hip.
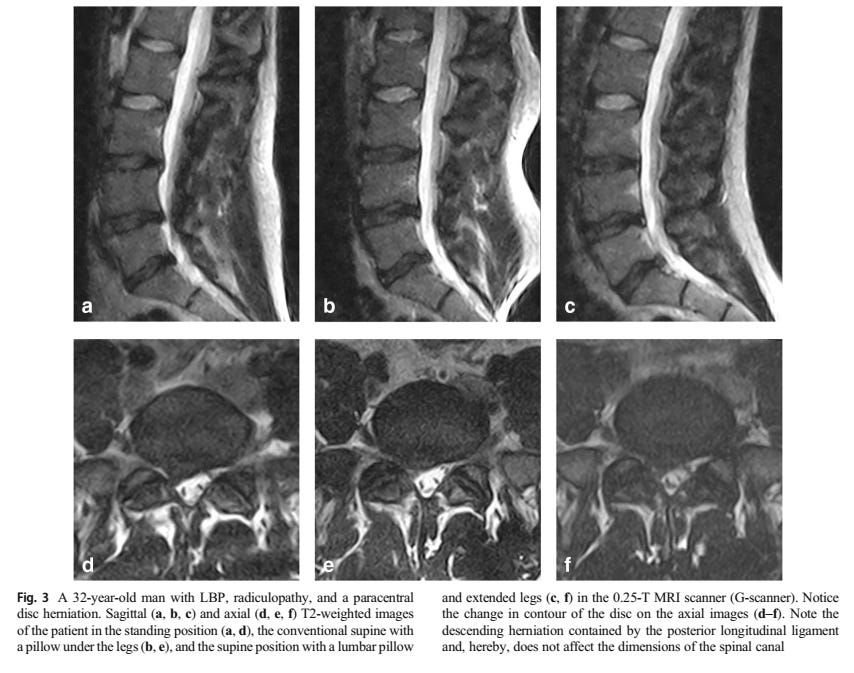
But, another recent study by Nordberg et al. gives some support to the "back people". They found that on upright MRI, disc herniations are bigger and nerve root compression is greater than in supine. The debate rages.
Predicting outcomes from surgery
Who does best from lumbar disc herniation surgery? Unfortunately, Willems et al. could not find an answer. They collected demographic, radiological and symptom data from 298 patients before surgery, but could not find any meaningful associations with outcomes. It's great to see a study published with "negative" results. They didn’t collect data on psychosocial variables, so maybe the answer lies there.
Disc regression
What more is there to say about lumbar disc regression/resorbtion after the excellent "the bigger the bulge the better" review by Chiu et al? Wang et al. reviewed the data again with some slightly different inclusion/exclusion criteria. They were able to shed a bit of light on how long disc regression takes.
Three studies with short term follow up (at 45 days, 20 days and 5 days) found no regression at all, suggesting the process takes a bit longer than a month or two.
They very loosely estimate that the average regression rate of 63% is reached at about ten months.
The very long term studies, over two years, are quite mixed (with rates of regression in the 50s, 70s, 80s and 90s) which suggests that even given a lot of time, many disc herniations will just stick around.


Picture from the recommended chirogeek.com
Who has neuropathic pain?
We commonly ask about things like numbness, tingling and pins and needles to find out whether someone has nerve pain. Heraughty and Ridehalgh conducted a systematic review to find out how good these descriptors really are at identifying who has neuropathic low back pain (which includes axial neuropathic pain, as well as radicular).
They found that self-reported allodynia (pain caused by touch that wouldn't normally be painful) and numbness seemed best. I was surprised to find spontaneous, paroxysmal pain was not that well supported.
I once gave a talk in Newcastle and suggested the acronym "SHAN" for identifying neuropathic pain: Spontaneous pain, Hyperalgesia, Allodynia, Numbness. I don't think SHAN translates that well outside the North East and Scotland. But apparently it should have just been "AN" anyway!
My impression from the review is that the evidence it draws on is quite limited. Especially considering all the issues with defining neuropathic pain.
Bits and bobs.
A survey on sciatica, please take!

I am working my way through Mark Laslett's online lumbar radicular syndromes course. It's really good, especially for the price. I've been meaning to take his course for a while because I think we have some quite different perspectives which I am trying to learn from. I will ask if he wants to talk for a podcast.
Next week I am going on Annina Schmid and Colette Ridehalgh's course, too (at 3am my time!). They have both kindly agreed to talk afterwards, separately, for two podcasts. I will look through the questions that have been submitted already to see if any would be good to ask. But if you have any questions in particular for Doctors Schmid or Ridehalgh please let me know.
I am DESIGNING A BOOK COVER! My sister, who is more talented than me, is helping. At the moment we are trying to turn the relevant bits of the nervous system into a more abstract or schematic pattern, which we will maybe screen print…
I’m still failing to keep these newsletters short, aren’t I?
I hope the research review was interesting! Are you a bum person or a back person?
Til next time,
Tom