
Sciatica Atlas 02
Three more notes

Thanks for subscribing to my newsletter on lumbar nerve root syndromes aka sciatica.
The Sciatica Atlas is a free, in-progress project covering the essentials of sciatica: what it is, how to assess it, and how to manage it in clinic.
While the site is being built, I’ll share the work here as short, memorable Atlas notes. Each note is meant to be vivid and teachable: stories, analogies, and mnemonics that make ideas click and spread.
Three sample notes are below.

1) The Danger is at the Shoulder
The cauda equina rests in the spacious thecal sac, cushioned by cerebrospinal fluid. The roots are well-protected in their nest. That’s partly why cauda equina syndrome is so rare.
But every root has to leave the nest. As it exits, it’s drawn into a narrower sleeve, and more tightly confined by bone and ligaments. Here, the risks begin.
The main threat is a disc herniation. In the lower lumbar spine, herniations tend to strike at a very specific point: the shoulder of the sleeve, just as the root leaves the sac.
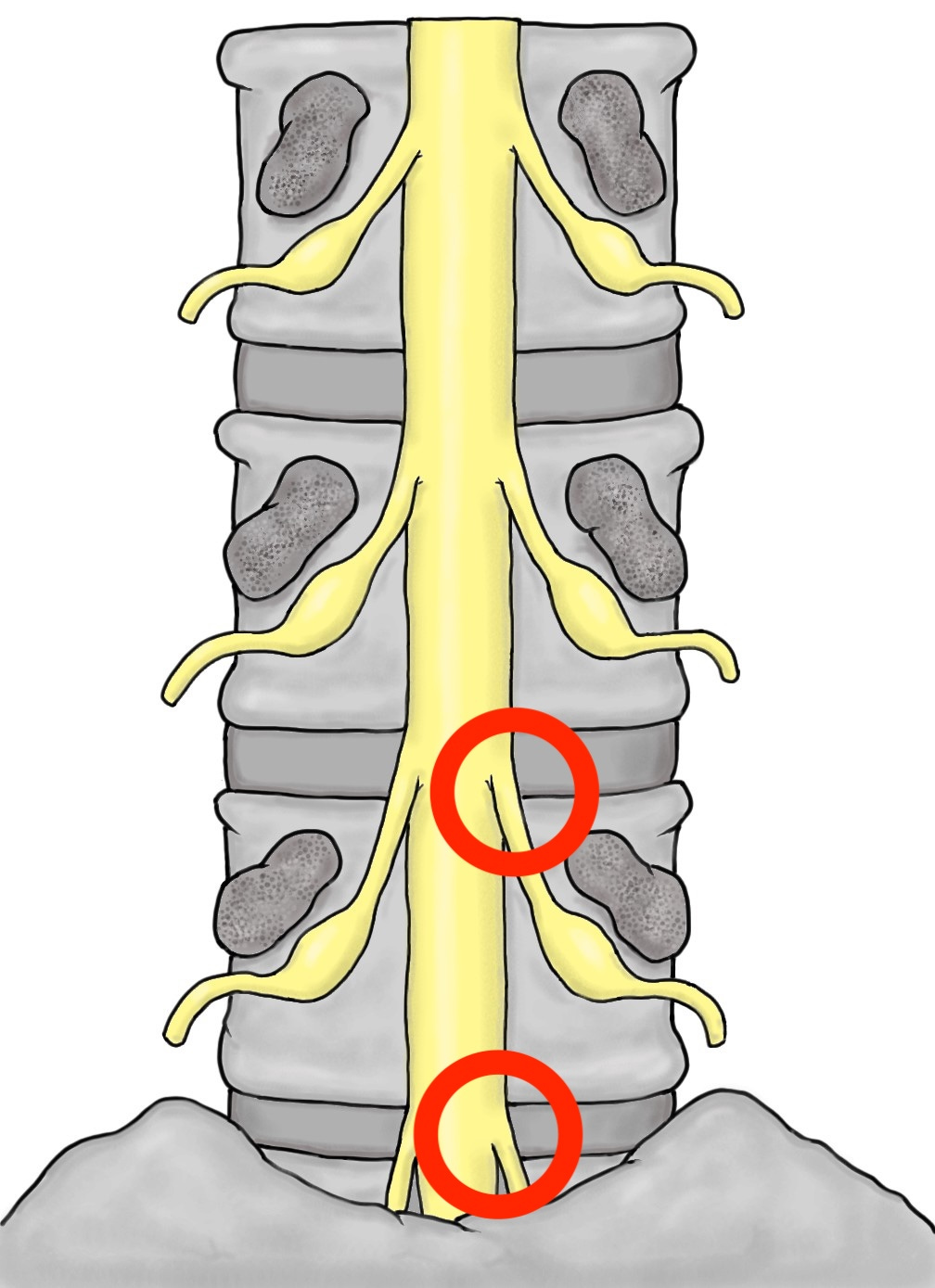
Further down the sleeve, trouble can still strike: arthritis, or a rare far-lateral herniation. But the shoulder is the the main point of vulnerability.
That’s why L5 symptoms dominate at L4–5, and S1 at L5–S1.
2) Grieve’s Dictum
For most people, under-loading the disc is a bigger problem than over-loading it.
We can look to new studies for proof: sedentary discs degenerate; moving discs thrive. Disc cells love light-to-moderate cyclic loading.
But we've known it for some time. In a 45-year-old textbook, Gregory Grieve put it better than anyone ever will: "The intervertebral disc lives by movement, and dies for lack of it".
3) Switched off vs bunged up
"I haven't been able to go for days"
A red flag for cauda equina syndrome.
Of course, it's probably just the codeine causing constipation. But how do you differentiate?
People who are just constipated feel full. They're uncomfortable, they want to go. And they can push and bear down. It's just nothing comes out. There's a plumbing problem.
People with CES affecting their bowel do not feel that sense of rectal fullness, as it’s called. And they can't push and bear down effectively. There's a wiring problem.
Of course, because nothing is simple: some people with CES might feel full, but be unable to bear down and vice versa; the loss of nerve function needn't be complete.
But the bottom line is still this: with constipation the bowel is bunged up; with CES the bowel is switched off.