


Timing for surgery, research review, turkeys

Thank for reading the second copy of my newsletter. I hope it finds you well. It’s later than intended so let’s get started straight away!
Does timing matter for surgery for sciatica?
You are seeing a patient with sciatica and they're not getting better. Or they're getting a bit better but not much better. Do you need to worry about *when* you refer them to surgery? If your next available appointment is in a month, can you wait and see how things are then? If waiting times to see a surgeon are three months, do you need to allow for that?
This is not about whether surgery is a good decision for the patient which is a topic for another day. It's about whether there is a window of time in which it is optimal to have that surgery
Schoenfeld and Bono set out to answer this question in 2015 in their review paper Does surgical timing influence functional recovery after lumbar discectomy? They found pretty consistent evidence that when people waited longer for surgery, their outcomes were worse. They say the evidence got much hazier when they tried to work out whether there was a particular cutoff point. But they reckon about six months.
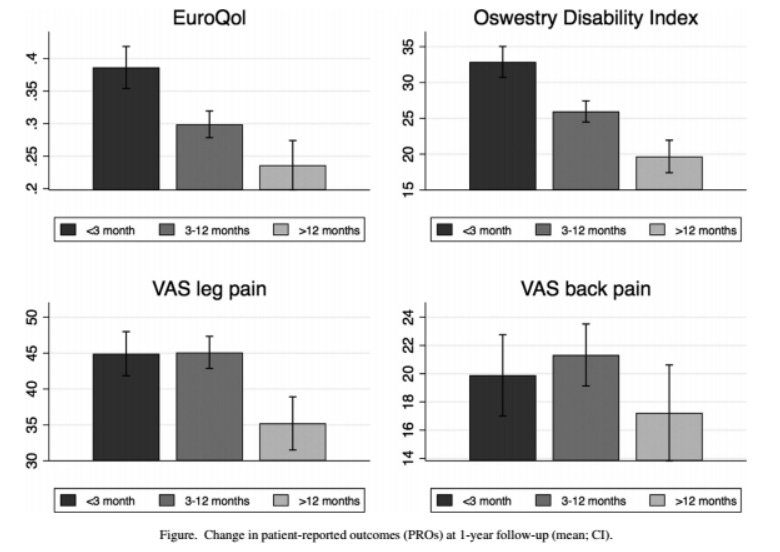
Since Schoenfeld and Bono there have been a few more studies which all said similar things. Siccoli et al looked back at the outcomes for 372 patients who had undergone microdiscectomy. They wanted to identify the cutoff point beyond which 80% of their patients weren't getting a meaningful benefit from surgery (meaningful benefit = more than 30% change in NRS). They decided the cutoff was 24 weeks - so, not too far off the six months Schoenfeld and Bono set.

As you can see from the picture, of the patients operated on after six months of pain, fewer had good outcomes. (But note the truncated y-axis - this difference isn’t *that* great).
Støttrup et al found someting similar last year. They split their data up a different way because of how things are categorised in their country. But again, that the longer people waited, the worse their outcomes (and more truncated y-axes):
As the last thing on this topic, I want to mention a really interesting RCT published in 2008 by Peul et al called Surgery versus prolonged conservative treatment for sciatica. Wilco Peul is from the Netherlands, where guidelines say you should consider surgery after six weeks of conservative care. But he noticed the UK guidelines said six months - very different! Essentially, Puel tested the two against each other. They found that after a year, outcomes were about the same. But, patients who got surgery early recovered quicker:

Note, this is *not* a trial of surgery versus conservative care! (I have actually given a presentation where I said this but it's wrong 😬). It is is a trial of two *strategies* of care: early surgery versus prolonged conservative care. In fact, 40% of the patients in the conservative arm did get surgery, after a median of 15 weeks’ conservative care, because they had intractable pain.
So, the pro-surgery spin on this would be "early surgery saves a lot of suffering and if you wait, lots of people still end up getting surgery." The anti-surgery spin would be "if you wait, you can save 60% of people from surgery and although they suffer more in the short term it doesn't make a difference in the long term." Peul speaks very well on this.
When it comes to answering our question on the timing of surgery for sciatica, I think this study says it’s okay to wait, but don’t wait too long. I found the following picture on google images, made by Peul. (I don’t have access to the full text). I think it is a great visual summary of everything I have written above:

Now, up til now I have not made the obligatory "correlation does not equal causation" caveat. But consistent correlations invite you to look for causation. And in this case, the correlations fit with what we know about biological mechanisms, too: that a nerve root that spends a long time in a crappy environment might sustain permanent damage, or that a nervous *system* processing nociception for a long time might just decide it's going to have pain forever now.
An important final point is that just because outcomes seem worse after six months does not mean that after this cutoff point surgery is contra-indicated! In fact, if you look at the data from the above studies, the proportion of patients reporting a favourable outcome isn’t *that* much lower after six months. (A NEJM RCT published just last month seems to support this.)
Research review (stuff that caught my eye)
As we know, disc herniations often spontaneously resporb. And, as the nun said to the bishop, the bigger the bulge the better. One guess as to why this happens is that the nucleus is seen as a "foreign body" to the immune system. So when there is a lot of nucleus splodged out all over the place, the immune system works much harder than it would for a regular old disc bulge and cleans everything up more thoroughly.

Djuric et al (along with Peul, mentioned for his RCT above) tested this theory by measuring the number of macrophages (gobbling-up cells) in extruded disc material. What they found supported the theory. Bigger extrusions had more macrophages. And the more macrophages, the more the extrusion reduced in size.

Nerve root entrapment causes autonomic dysfunction, which causes temperature changes. Park et al. reckon that in more acute, traumatic and severe cases you get hyperthermia. In more chronic cases, hypothermia. (Like CRPS?)

Wanderman et al: "Herniation occurred outside the spinal canal, leading to marked inflammation of the adjacent muscle [psoas], manifesting as myofascial pain syndrome." Who’d have thought?
Finally, a new Cochrane review of injections for lumbosacral radicular pain concludes, "Probably slightly better than placebo in reducing leg pain and disability at short-term follow-up. However, the treatment effects were small and may not be considered clinically important by patients and clinicians". I have yet to read it properly.

Other bits and bobs
Chris Littlewood, Nadine Foster and I had a letter to the editor published in JOSPT about a shoulder pain systematic review. For whatever reason, it is the only letter to the editor in JOSPT's history that they have ever put behind a paywall. Here's a link though.
I made this "masterclass" thing for Physio Network. I didn't realise they were going to use my fat face for an aggressive Facebook marketing campaign 😆. If you are a Facebook user, sorry.
Doing the masterclass was a good way to push myself on to the "next level" on this topic. Which has gone from tweet thread —> magazine article —> local talks —> conference talk —> podcast —> masterclass —> ???. Basically, my tactic has been "commit myself to something I'm not quite able to do yet and step up to it". I recommend this.
My green card interview is postponed indefinitely because of 🦠COVID! But as my dad would say, worse things happen at sea. And if this is the worst thing to happen to us because of the virus we will have done alrigh (I almost went the whole newsletter without mentioning COVID…).
It's getting on for turkey season in Michigan 🦃🦃. Wild turkeys are gigantic, fearless dinosaurs. One just walked past our window. This was quite intimadating because we live in one of those semi-basement apartments so it was about two feet away looking *down at me*.
That’s it for this edition. Thanks for reading! I got a some really encouraging replies to the last newsletter and some interesting questions too. Do get in touch.
🧍Happy🧍social🧍distancing🧍,
Tom