
Why would sciatica take a fortnight to kick in? Pt 3.
Disc material, neuropathic pain, the CNS and final thoughts.

Thanks for reading the 37th edition of my sciatica newsletter. This newsletter tracks my research as I write a book about lumbar radicular pain!
Unfortunately Substack doesn’t allow me to send really long emails. So I’ve split this piece into three; this is the final installment.
Part 1 is here and part 2 is here.
Disc material also causes delayed loss of nerve function
As I mentioned, disc herniations can injure nerve roots not only through mechanical pressure but through chemical irritation, too. The insides of a disc seem to be inherently irritating to neural tissue. And in fact, the time-scales here also seem to be in days and weeks, rather than just hours. Maybe chemical irritation by disc material explains delayed-onset radiculopathy?
An experiment by Olmarker and colleagues suggests it could. The researchers applied nuclear material from pigs' discs to those same pigs' nerve roots (they were careful to merely apply the material to the roots, without adding pressure). In a control group, they applied fatty tissue instead. In the group of pigs whose nerve roots had been exposed to disc material, Olmarker and colleagues found signs of nerve degeneration after one day and three days, and these signs became more pronounced after seven days.
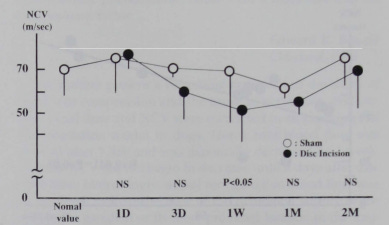
In another study, Otani and colleagues made incisions in the annulus of dogs' discs, allowing nuclear fluid to leak out:

They observed a decrease the conduction of action potentials through the nerve, which started on day three and peaked one week after the incision had been made.
Finally, Sakamoto and colleagues compared the effects of disc material to the effects of nerve compression in rabbits . They found that nuclear material was a bit slower than compression to cause a conduction block, not really getting going for a week.

So here is another potential explanation for this picture of delayed-onset post-herniation radicular pain: disc material apparently can take a little while to incite an inflammatory reaction and cause a conduction block through a nerve root.
How should we think about all this inflammation and degeneration? Kind of good and kind of bad
So far, I have mentioned these things ‘inflammation’ and ‘degeneration’ a lot. It's worth noting that all this inflammation and degeneration probably occurs somewhere at the border between an unwanted pathological process and an adaptive, physiological one. It’s like there are two sides to the story:
On the one hand, inflammation and nerve degeneration occur because, as I said above, neurons are starved of oxygen and nutrition or exposed to harmful disc material. This seems particularly true for very severe injuries, which cause relatively quick, pathological and disorganised harm to nerves: neurons and Schwann cells simply can't survive in a high-pressure or very inflammatory environment.
On the other hand, inflammation and nerve degeneration are just part of the immune system's response to danger. This seems particularly true for very mild injuries, which can cause a weeks-long, apparently controlled, 'deliberate' process of demyelination and remyelination, accompanied by a gradual infiltration of macrophages (clearing-up cells), all without any axonal degeneration underneath. Degeneration precedes regeneration.
I freely admit I don't really understand this thing about inflammation and degeneration being kind of good and kind of bad. I need to work harder at it. The point is that, whether this process is good or bad, it is a process, which takes time that can be measured in days and weeks, and so potentially explains a delay in radiculopathy after the initiating injury!
Some neuropathic pain processes also take a while to build up
The above studies only measured conduction loss of nerve root function, not pain. So why might nerve root pain have a delayed onset?
One way to think about this is that, after injury, a neuron has to undergo some change to become capable of generating the ectopic impulses that seem to cause the sharp, severe, shooting symptoms of radicular pain, and possibly also cause much of the background burning ache.
After all, the axon of a neuron, as it passes through the nerve root, is only supposed to conduct impulses, not generate them. This is why prodding and pulling uninjured nerve roots does not produce radicular pain. In order for a nerve root to become sensitive and generate impulses, a whole pathological process has to play out in which ion channels become embedded in the axon of a neuron where they are then capable of generating those ectopic (i.e. 'in the wrong place') action potentials.
Ion channels can bunch up and create these hot-spot ectopic sites in response to frank nerve injury and demyelination:

This is the classic understanding of neuropathic pain put forward by Marshall Devor, among others. In his chapter in the Textbook of Pain, Devor shows that these sites tend to build up and increase their firing rate on a scale of weeks rather than days.

This slow accumulation of ion channels to form hot spots that generate ectopic impulses partly explains that late-onset of nerve pain generally, which I mentioned earlier - and perhaps it partly explains the late onset of mine and Adam's radicular pain.
It's worth saying that it is not only frank nerve damage and demyelination that can cause hot spots to develop, but also mere inflammation, too. The work of Dilley and Bove demonstrates that inflammation impairs axonal transport of ion channels, which makes them bunch up and lodge abnormally in the axon:
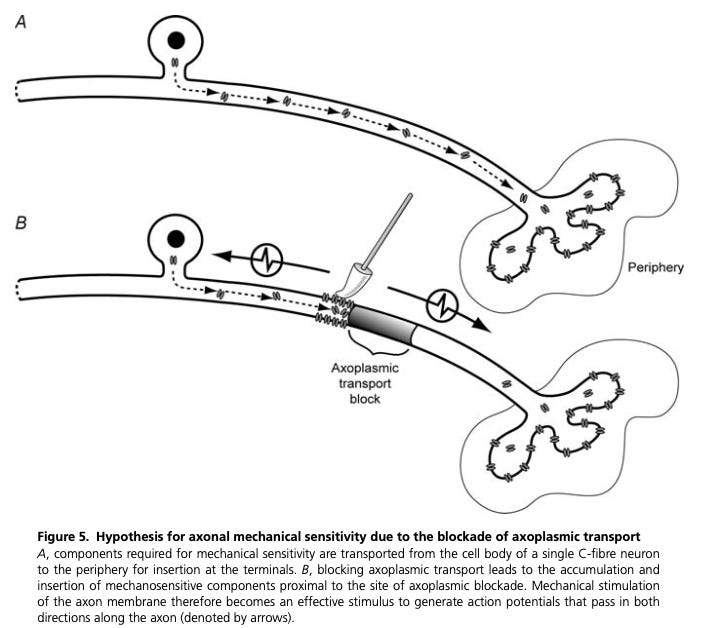
In their study led by Satkeviciute, they found that in mice this process takes four or five days to peak (perhaps longer in humans?). Here again is another potential explanation for late-onset radicular pain.
Put this way, it does not seem too surprising that radicular pain could come on a couple of weeks after the initial injury.
Could the CNS explain it?
Finally, let's zoom out from the nerve root and think about the whole CNS and the whole person. I think this is where things get (even more) hazy and you can start coming up with endless hypotheses for why radicular pain might have a latent onset. So I will just note a three quick things that seem plausible to me. Please do not read on if you are sensitive to simplified language and neuro-fallacies.
Maybe back pain somehow 'suppresses' radicular pain? Maybe for Adam and me, our nerve roots started firing off ectopic impulses quite early but our brains' great inner Eye of Sauron was just focused on the back pain. Maybe the back pain started to ease off just a bit and all of a sudden the radicular pain was 'noticed'.
Maybe back pain gradually sensitises the system to radicular pain? The stress of back pain, along with the lack of sleep and so on, might sensitise a person's system so that danger messages from a mild nerve root injury eventually become noticed after a week or so, even though the messages themselves haven’t changed.
Maybe it takes some time for CNS to undergo a process of disinhibition to ectopic impulses from the nerve root? The nervous system ordinarily inhibits the bombardment of sensory input that is always coming in from nerve endings. When a nerve is injured, the nervous system lifts some of this inhibition. Although these processes are as welldocumented as they are difficult to understand, I found it surprisingly hard to find any information about how long all this stuff generally takes. Perhaps we are looking at days and weeks here?
It's worth noting, however, that none of these points fully explain late-onset loss of strength and sensation.
In summary….
How can I summarise all this speculation? Let's try
If radicular pain comes on later than back pain, it could be because of a subsequent change in the disc: perhaps the disc has herniated gradually, or a fragment of the herniation has migrated.
On the other hand, it could be because of (patho)physiological processes in the nerve root that, after a disc herniation, take a week or two to get going.
These processes might include gradually-building inflammation and associated nerve degeneration, perhaps in response to mild compression or to the presence of nucleus pulposus; and gradually-accumulating ectopic impulse ‘hot spots’.
Of course, it could be that past a certain point, whatever is happening in the disc or the nerve root is moot and that the delayed onset is to do with shifting 'attention' or delayed disinhibition of the CNS.
And it goes without saying that none of these explanations are mutually exclusive - they could all be going on!

And finally I would suggest a few clinical conclusions, by no means an exhaustive list:
A delayed onset of a nerve root problem doesn’t necessarily mean ‘another thing has gone wrong’.
A delayed onset of a nerve root problem could be part of the body’s natural process of responding to injury by 'clearing out’ some of the old nerve tissue so that it can put some new tissue back in.
The fact that delayed onset of a nerve root problem is possible, and maybe even expected, is evidence in favour of the argument that we should ‘safety net’ people with low back pain alone (i.e. no sciatica) for CES
“Every ‘simple’ backache has the potential to be a nerve root problem” - Louis Gifford
That’s it! I’m really interested in your thoughts and impressions on this post. Feel free to contact me - just hit reply to the email. Or, you can comment on the post on Substack: