

Thanks for reading the 55th edition of my newsletter. This newsletter tracks my work on a set of books about lumbar nerve root sydromes. Current status:
Cauda Equina Syndrome book: Finished 🏁
Sciatica book 1: Being reworked and rewritten for paperback 🔃
Sciatica book 2: In progress 🚧
Welcome new subscribers from Todd Hargrove’s excellent newsletter.
I spoke to Todd for his podcast this week, the link is here. We started by talking about writing and building knowledge. Then I played some of the hits about definitions of radicular pain, radiculopathy and referred pain… Then I picked up on some of the finer details about radicular pain, including plenty of self-contradiction and some unsupportable speculation (always fun). I try not to make excuses for things but I feel like I might have had a touch of ‘tired dad brain’ for this one! Nevertheless, Todd assures me it’s a good listen :)
Next, some news. As readers know, I am reworking the first sciatica book, on pathomechanisms. And I’m very pleased and proud to say that I’m being helped in this task by Annina Schmid. I’m very proud of this book but with Annina’s help it is improving significantly, and I hope it will be the text on sciatica for many years to come.
Okay, this week I thought it would be interesting to talk about some insights I have learned about sciatica from people with sciatica (i.e. radicular pain!) I’ll also suggest a few things we can do to act on those insights.
Necessarily, this is only a partial list and somewhat random, based on some ‘learning moments’ in my own career… You should let me know what you think is missing. What have you learned from your patients that you didn’t get from textbooks and school?
1. It can be really, really bad.

This might seem obvious on the face of it. Of course sciatica is bad! But it’s worth pausing to (try to) appreciate just how really, really bad it can be. It took me a long time to realise this…
Certainly this patient, quoted in a qualitative paper by Ryan and Roberts, thinks that clinicians don’t really get it:
“I feel like people have got no understanding of just how painful it can be. I don’t think it’s taken seriously enough. I don’t think people realise how painful it is. It’s excruciating, constant”
In that paper, three out of 14 people said they’d contemplated suicide.
If (like me) you’ve never had really bad neuropathic pain, it’s hard to imagine it. After an unsuccesful operation for his sciatica, the epidemiologist Jonathan Mayer wrote evocatively:
‘I’ve heard patients ridiculed in team discussions if they report a level of seventeen on a ten-point pain scale, but I discovered what those patients must mean. They were communicating feelings of loss of self, of being a screaming animal reduced to the level of mere survival. They were trying to emphasise that the pain was not just as bad as they could possibly imagine but worse than they could possibly imagine’
(The whole piece is great)
Of course, radicular pain isn’t always quite that bad. But, it’s worth considering that it is, for some people…
Okay, what can you do about that?
Acknowledge the pain and ‘bear witness’. I know, it’s not going to have your patient dancing out the door. But there’s sometimes some magic that happens when a clinician really ‘sees’ a patient’s pain.
Personally I have experienced this magic before, as the patient… I still remember the relief I felt when I heard that nurse say to herself ‘Wow, this guy’s really suffering!’ (I also remember the deep frustration and sadness I felt the other clinicans I’d seen before her didn’t appear to understand).Explain that the pain is common and does not in itself mean there’s a more serious problem. Help your patient understand a bit about the assessment you’ve done and why it strongly suggests there’s nothing more serious to worry about than the pain. You’re trying to minimise the ‘but what if the physio missed something’ voice in their head, which can only make things worse.
Give ‘go getters’ permission to rest, early on.
Don’t under-use short-term pain relief. Our MSK clinicians’ bias against injections and operations can be unhelpful sometimes.

2. The ‘nervey’ symptoms can be frightening.
Here’s another patient from the study by Ryan and Roberts:
‘When I think about my leg I can feel the pins and needles going down it and the pain, and I’m sure it’s all in the mind’
As clinicians, we’re used to hearing about tingling, pins and needles, patches of numbness, hot legs, cold legs, feelings of running water… But our patients aren’t prepared for these sensations.
‘The pain and associated symptoms such as numbness and tingling are frightening for patients, especially if they do not understand the cause.’ (Ong et al.)
What can you do about that?
Explain that the unusual symptoms are common. Let your patient know you’ve seen this before, plenty of times.
If you are comfortable doing so, you can also say something about why they happen. There’s no script, but how about this: ‘The nerve sends signals up to the brain about what is going on around you. Those signals tell your brain when something is hot, or cold, or touching you or moving on your skin. But when there is a problem in the nerve, it starts firing off all these wrong messages, sort of like white noise… So you feel like something’s prickling you when it isn’t.’Draw on everyday experiences to make the sensations feel more normal. Most people know that if they sit awkwardly then their leg goes numb and they get pins and needles. ‘It’s not too different to what I think’s going on with the nerve in your spine. It’s likely getting crowded out so it doesn’t get the blood it needs, which is making your skin numb and tingly…’

3. People really want to know what’s going on.
Here are two different patients:
‘If I just know myself what’s going on…, I could probably deal with it myself as effectively as taking half a day off work to go and sit in the GP surgery to get given ibuprofen or some other tranquiliser that I don’t want to take’ (patient quoted by Goldsmith and colleagues)
‘Even if they can’t deliver a solution, imparting a good element of information to the client can be part of the remedy in its own way’ (patient quoted by Ong and colleagues)
Both of these people know they need a better idea about what is happening to their bodies so they can make better decisions about what to do and how they should feel.
What can you do to help?
Well, explain what’s going on!
Of course, don’t explain anything without first listening carefully for as much time as you can afford. Then, ask the patient if they do in fact want an explanation (some, of course, couldn’t give a hoot). If they do, explain by ‘meeting patients at their understanding’. Draw on their own symptom patterns, use words they use (even if they are not technically ‘correct’).
Start with even more basic information than it feels like you should – what is a nerve? Even if your patient knows what a nerve is and what it does, saying it all out loud acts as a shared understanding and serves as the foundation of your explanation. Use a spinal model if you have one. They are falling out of fashion but in my opinion they are a great prop.
If you aren’t sure in your explanation, well… the book will be out soon! :)
4. People think it’s all to do with compression - ‘trapped’ and ‘pinched’ nerves.
Which is unsurprising, since many healthcare professionals do, too…
It’s true that pressure has some role in radicular pain, but it can’t explain the whole picture. After all, the size of a disc herniation often doesn’t match the level of pain our patients are feeling, and some people have no apparent herniation at all.
A big missing piece of the picture is inflammation.
Why does it matter that so many patients think sciatica is all to do with compression? Well, if you think that pain = a nerve being squashed…
You’re unlikely to want to move at all
There’s no real reason to do anything except hope for an operation (as one patient says, quoted by Goldsmith and colleagues, ‘just get in there and sort this!’)
If/when you eventually get an MRI and, as often happens, it doesn’t show compression of the nerve root, then you’re really lost. (As one patient said, ‘the specialist [who reported the MRI] really cut my wires on that one’.)
So what can you do to help?
Consider a ‘two-step’ explanation.
Explain to your patient that something is likely crowding out and bothering your their nerve. (Although we like to avoid structural explanations for pain these days, I don’t think it’s helpful or accurate to say that there’s no structural cause of radicular pain. Very often there is.)
Explain that as a result, the nerve is also sensitive, irritated, sore, inflamed, pissed off - whatever word feels best. ‘Nerves are made of tough stuff, but they' don’t like being crowded out and they sometimes react irritably’. Whatever helps to introduce the idea of soreness and sensitivity of the nerve as well as just compression.
Of course, there are some ways in which this is over-simplistic. But I think it is a nice way to set you and your patient up for success without attempting to completely overhaul their preconceived ideas of sciatica, and pain in general. It opens the door to an understanding of factors beyond the nerve root, too; many people find that stress and sleep have a strong effect on their symptoms.
5. People can end up with their life on hold.
Saunders and colleagues say that people with sciatica ‘are caught between their pre- and post-sickness selves, unable to fully identify with either.’ They use the phrase ‘biographical suspension’ to describe this.
As an example, here is a patient with a one-year history of sciatica:
‘It’s as if everything stopped August 12th. But I know [my health] will come back’
Ryan and Roberts use the phrase ‘life on hold’ to describe a similar idea that people with sciatica often get stuck waiting for their life to start up again.
What can you do to help?
Balance optimism with realism.
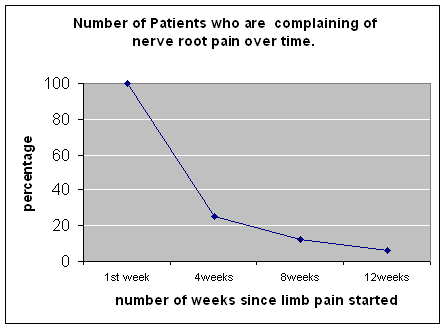
On the one hand, there is every reason to be optimistic about an acute onset of sciatica. According to one trial, after three months, about half of people are much better or completely recovered. After a year, it’s three quarters. Not great, but not bad either.
On the other hand, that means that for about a quarter of people, sciatica is still a problem after a year. For many, the problem will be very serious. So we should balance our optimism with realism, and be alert for patients who aren’t improving with time so we can adjust our message accordingly.
Here’s an example of a message I think is too opimistic. This graph, from a spinal surgeon’s organisation, implies that 95% of people will be better after 12 weeks!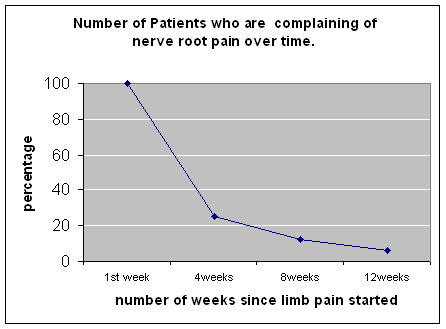
I hate to imply that striking this balance is easy. It takes experience and wisdom to help patients to navigate the possibility that a problem they thought was going to get better might, in fact, persist. I don’t claim to be good at it. But the simplest thing we can do is give good information.
On her excellent blog livingwellpain.net, Tina Price says that ‘I think clinicians should be more honest from the beginning when they know there could be a chance of long-term pain. Mine weren’t.’Try to make rehab participation-based.
There’s nothing wrong with specific, anatomically-reasoned exercises like nerve sliders and gliders. For lots of patients, they’re fantastic (although the evidence is lukewarm). But in my experience too many patients are given little else except ‘fiddly physio exercises,’ which doesn’t seem like the best way to help them to take their life ‘off hold’.
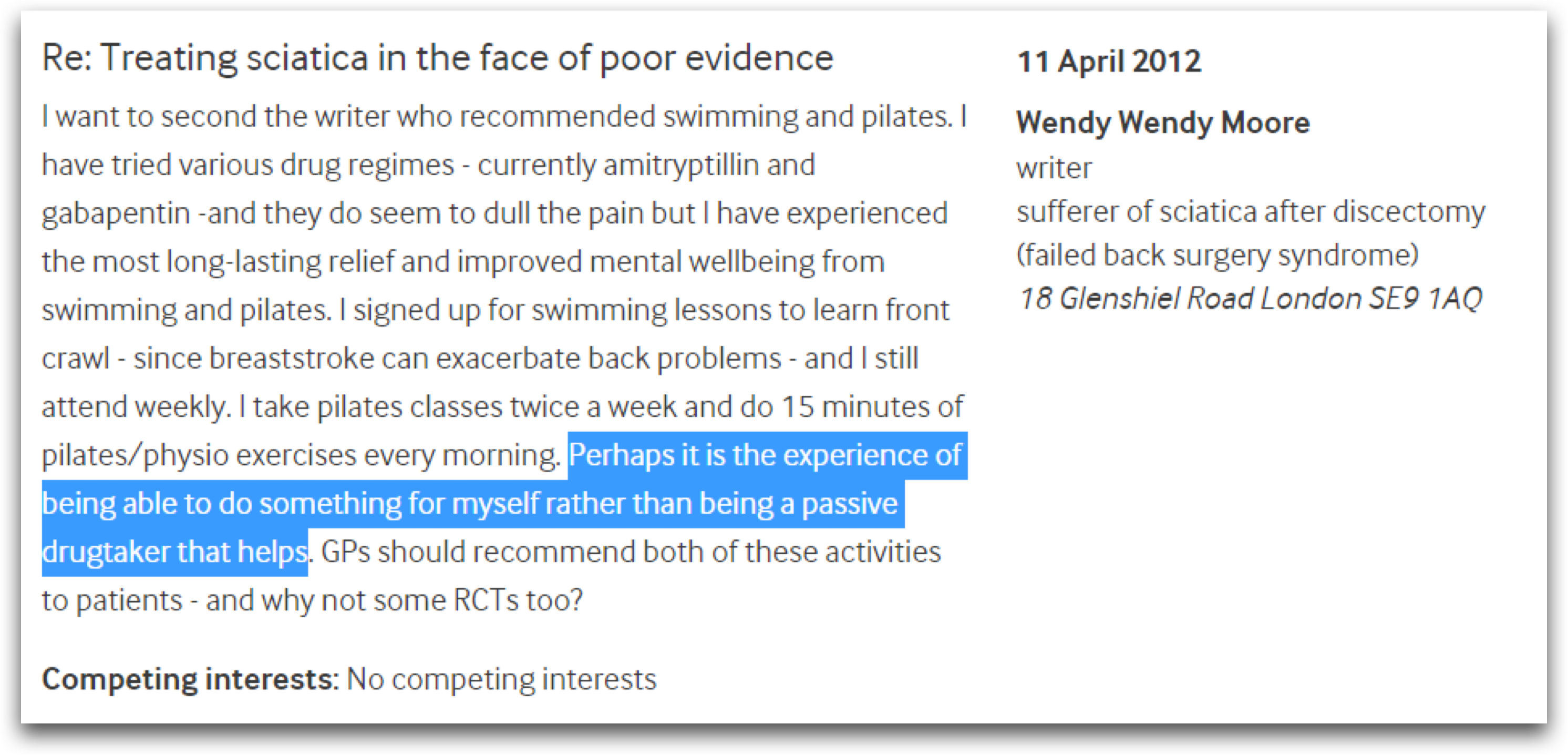
So I think we should also (or rather) help patients to get back to things they want or need to do. This commenter on the BMJ website found that it’s enjoyable general exercise that helps her:
…So there you have it. Five insights we can take from patients!
Again, this is only a partial list, mostly based on some ‘realisations’ in my own career. What do you think I’m missing? Let me know what you’ve learned from your patients.
I’m really interested in your perspectives on this one, including disagreements!
If you are interested in more stuff like this, maybe a good place to start would be the ‘for HCPs’ section of Tina’s blog.
Til next time,
Tom
P.S. If you still haven’t got your copy… www.theCESbook.com :)
