
Sciatica Atlas 03
Three more sciatica notes

Thanks for subscribing to my newsletter on lumbar nerve root syndromes aka sciatica.
The Sciatica Atlas is a free, in-progress project covering the essentials of sciatica: what it is, how to assess it, and how to manage it in clinic.
While the site is being built, I’ll be sharing the work here as short, memorable Atlas notes. Each note is meant to be vivid and teachable: stories, analogies, and mnemonics that make ideas click and spread.
Three sample notes are below.

1) Many roots make light work
When you sit wrong on a park bench, your foot feels completely dead. Numb and floppy. Peripheral nerves are like cables to a TV: if the cable doesn’t work, the TV goes dead.
But think about your patients with nerve root compression: they're weak, maybe a bit numb, but rarely completely ‘dead’ like that park bench foot.
It's because nerve roots are shuffled in the lumbosacral plexus. By the time each axon is in a peripheral nerve - the sciatic nerve, the femoral nerve - it's running alongside axons from several different roots, all braided together.
So there's a redundancy across roots. When one isn't working, there are others in the same peripheral nerve to pick up the slack. Lose L4, for example, and L2 and L3 can still contract the quad, albeit with less power. Many roots make light work.
One movement, though, doesn't quite have enough redundancy: dorsiflexion. Lose L5, and L4 is still there but sometimes can't generate enough power to get toe clearance. That's when you get an L5 foot drop.
2) It ain’t what you do, it’s how much you do it
A rehab rule-of-thumb: it ain’t what you do, it’s how much you do it. Different rehab approaches - core exercise, neurodynamics, general exercise - show similar results on average. The dose makes the medicine.
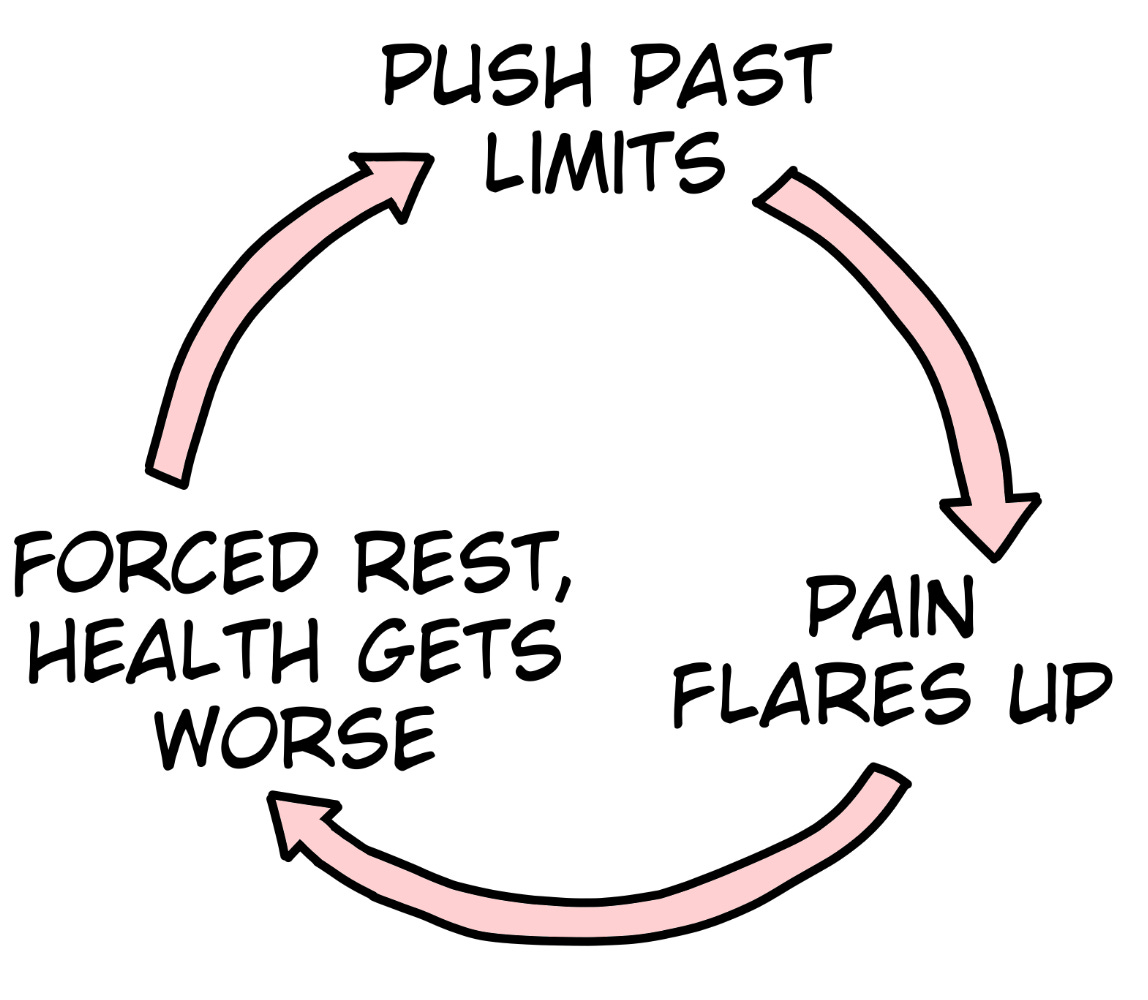
Don't do too much:
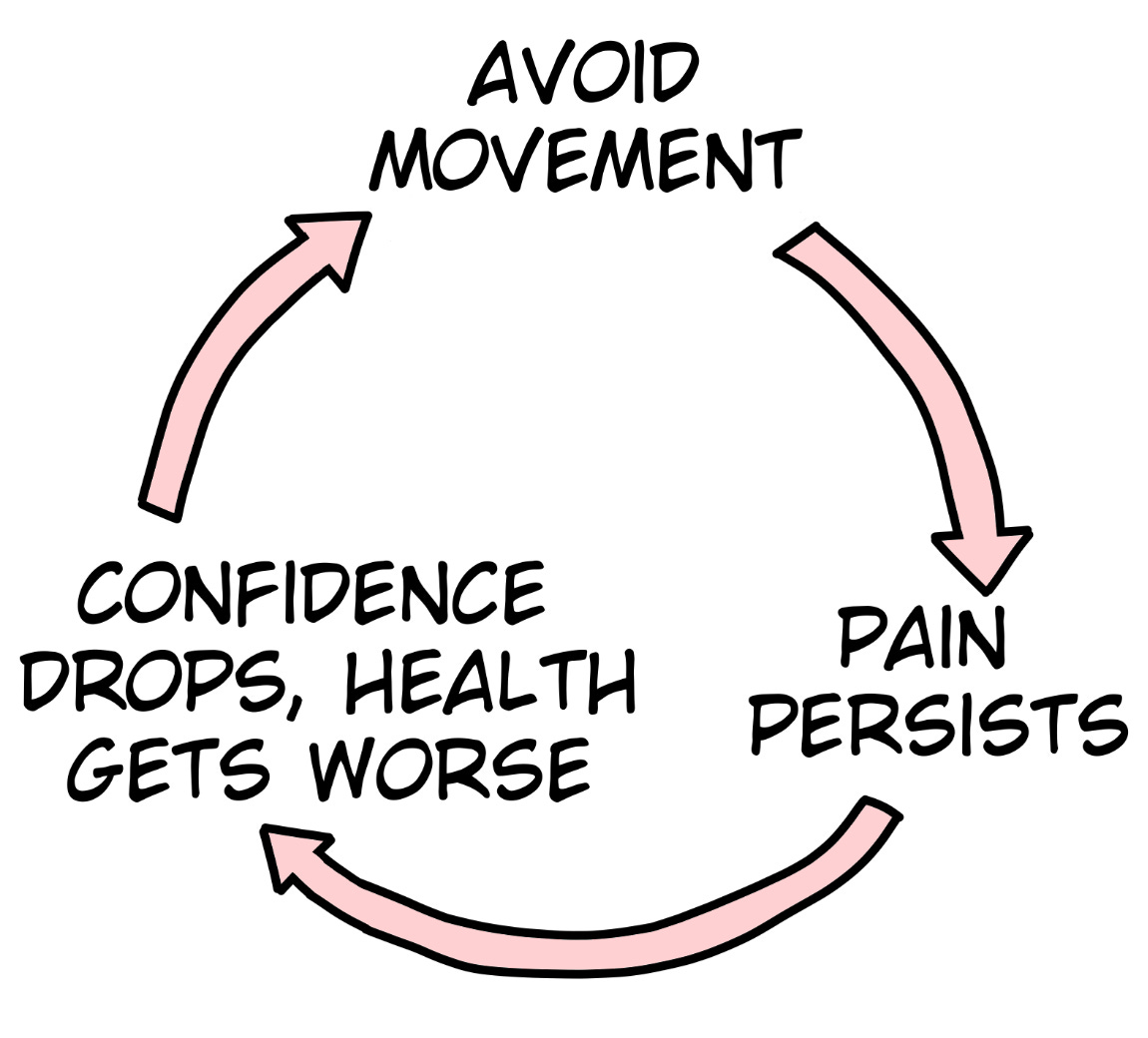
Don’t do too little:
And aim for the sweet spot: exercising within tolerable pain that doesn't flare up afterwards.
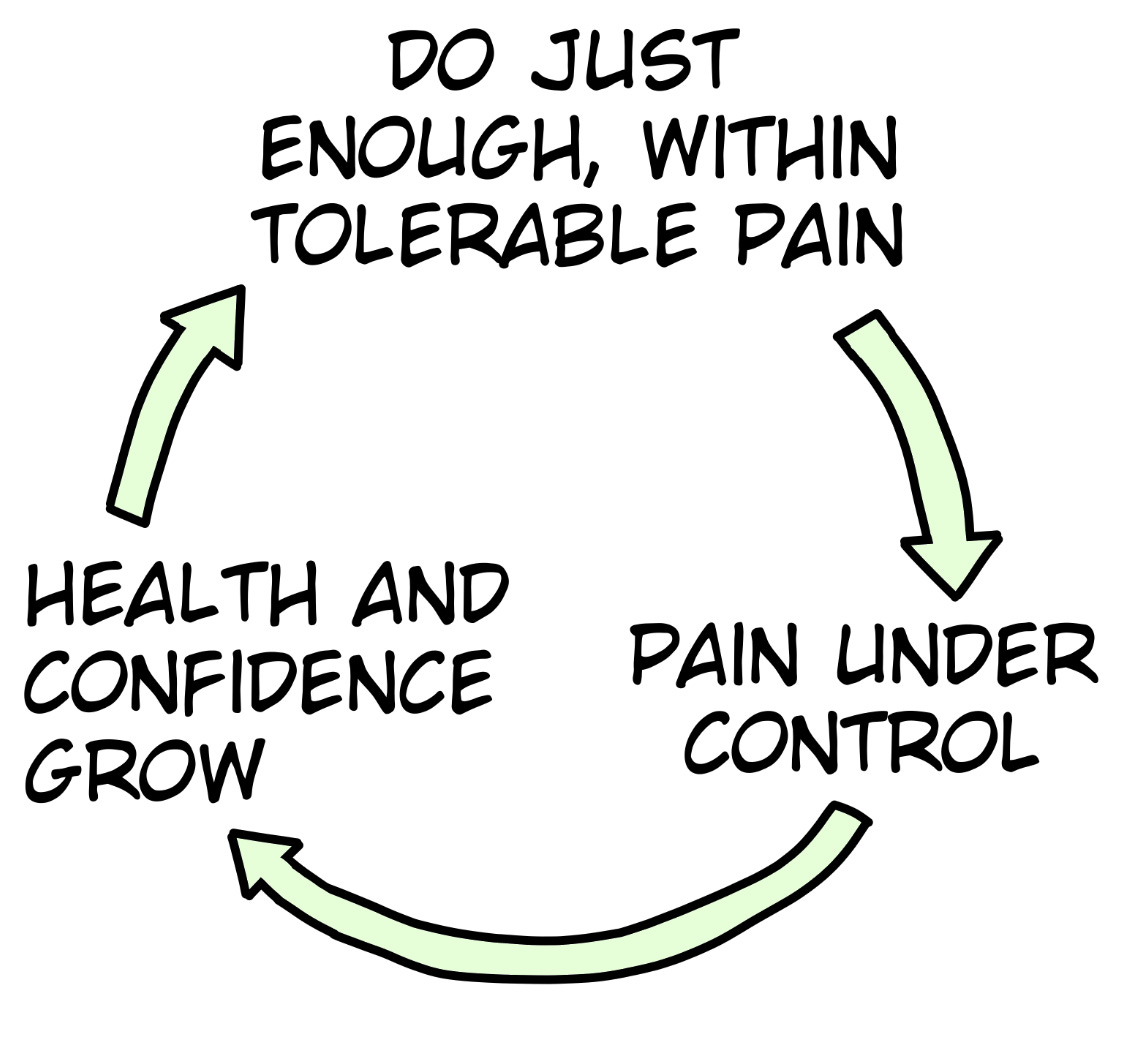
An even keel is the ideal.
3) Prognostic misconceptions
Three things that matter less than you might think:
The size of the disc herniation or the degree of nerve root compression. Big extrusions are bigger injuries, which is bad, but they're also more exposed to the immune system, so they're cleaned up more quickly. This trade-off means that big and small herniations share comparable prognoses.
The neurological deficit. Non-progressive sensory loss, reflex loss or weakness don't mean a patient will do worse.
Age. Younger people might do a bit better, but the advantage is minimal. Older patients face no inherent disadvantage.
Thank you for your helpful spirit. 🎈
Great explanation Thankyou