


What makes a good clinical book
And how we've made our CES book as good as possible

Thanks for reading the 48th edition of my newsletter. This newsletter tracks my research as I write a book about sciatica, and another one (out next) about cauda equina syndrome.
This week I want to share my ideas about what makes a good clinical book. This topic has been on my mind for a long time, but I've never actually written down my thoughts.
I’m not sure how many people will be interested in this ‘shop talk’, let’s see? I do think it might be helpful for people to read so they can reflect on their experiences as a reader and also on their own writing and communication….
As always, tell me if you think I'm missing something, or you disagree!
So, here's what I think a really good clinical book should be like, and how we’ve tried to make our CES book as good as possible.
Useful.
This sounds obvious. Useful is good! But, in my opinion, most clinical writing is not primarily intended to be useful.
For example, most journal articles and textbooks are primarily aiming for some other quality, like rigour or comprehensiveness or equipoise or authority.
Most blogs are primarily aiming to persuade or provoke or entertain. These are all good things but they often actively undercut the usefulness of the piece of writing.
We're lucky with the CES book because we can write it however we want. We don't need to conform to academic standards or attract clicks on Facebook. So we focused on making it useful.
Hopefully in the rest of the points I'm about to make, you'll see how each is underpinned by the primary goal of being useful. But here's a couple of little examples.
For one, we've written the chapter headings to 'give away the ending'. Chapters are not written like a mystery novel where you have to read to the end to find out the answer. We tell you the bottom line on the top line. Amongst other things, this should make the book more useful to browse and skim, and the key messages more memorable. Here's an example of some chapter headings:

Another example of how we've made the book useful is that we’ve focused on all the little things you need to do to get the big things right. For example, rather than just talk about clinical reasoning, we've explained how to clear time to think during your appointment so you can do that reasoning in the first place. Or, rather than just talk about referring patients to A&E, we've explained what to do when they don't want to go, or when they go but don't get seen. In my opinion, mediocre clinical writing often doesn’t do this, and instead just points you vaguely in one direction or another, sort of like an Ikea manual that says 'assemble furniture competently and in a timely manner'.
And as a final example, in order to make the book as useful as possible we’ve stringently left out all the useless stuff that often clogs up clinical writing. So there are no mini literature reviews where we say 'this study said this, but this study said that, and then this study said that'. There's also not much information on anatomy and pathomechanisms, and the information that is there is 'need-to-know', directly linked to an insight we want to convey.
Crispy.
I think one of the biggest problems in all clinical writing is vague, soggy words that point in the general direction of something good without really meaning anything concrete. Soggy words and phrases like 'patient centered', 'good quality rehab', 'reassurance', 'empathy' and 'clinical reasoning' sound nice but, in many contexts, don't actually mean much. Instead, a good clinical book should be full of specific, vivid, crispy detail.
For instance, here's a crispy detail about asking patients about a loss of saddle sensation:

...and another one on referring patients to A&E:

The value of 'crispiness' extends to the topic of the book itself. 'Potential CES for MSK clinicians' is a clearly-defined and manageably-sized crispy topic to write a book about. 'Sciatica'... is not. Which is why Book 2 is taking so long. If I could start again I would reduce the scope.
Visual.
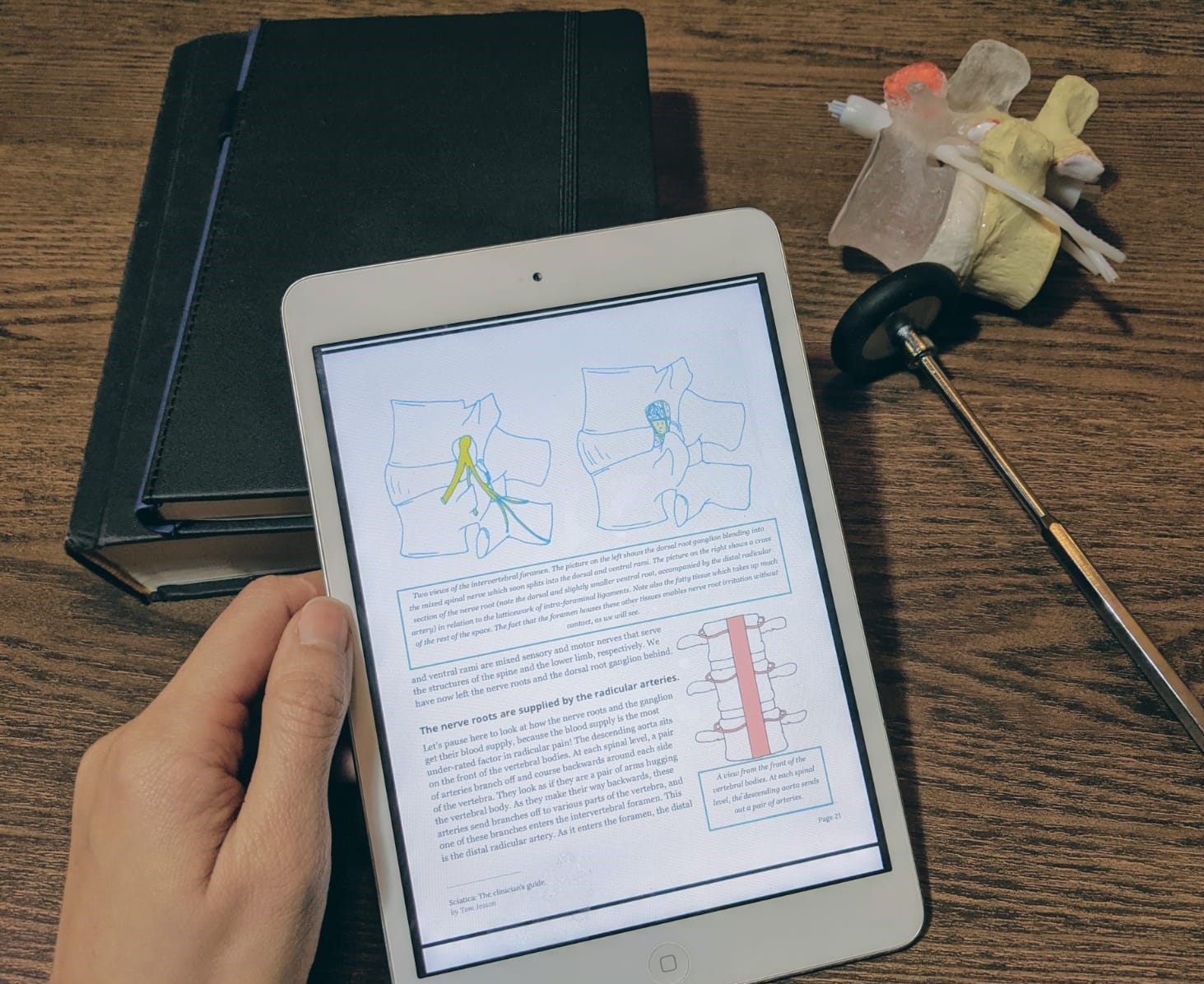
This is one thing we struggled with. The first sciatica book offered lots of opportunities for lovely illustrations.
")
The CES book has much less anatomy in it so it was difficult to know how to give it a visual element. For a while we thought we might illustrate the concepts with cartoons but our attempts looked amateurish and they didn't add much. In the end we've decided to include what I'm thinking of as visual knowledge summaries—basically recaps of each section but in a more visual way 1.



I think these visual summaries are effective. They don't look great though. I'd like to make future books look a lot prettier. It's just beyond my ability to do so at the minute.
I do think the cover is nice though.

Tested.
Every writer gets someone to read their work before it's published. They ask experts to fact check their document and ask/pay other people to proofread it for typos etc. But they rarely get the target audience to read it, and even more rarely give them the right conditions to give useful feedback.
I got the idea for test readers from a guy called Rob Fitzpatrick. He's from the product development world and he takes a similar approach to writing a book as he would for building software or an app. You do part of it, get the people who are going to use it to test use it, see how they do, and adjust accordingly. Repeat until all the test users are happily gliding through your software, app or book.
With the CES book, we have sent a copy of the manuscript to about 40 people, from students and new grads to FCPs, and given them time to go through it, highlighting what they liked in green and what they didn't like in red, and commenting with whatever came into their heads.
After going through the test reader process, I can't believe it isn't normal for every writer to do this. It seems like a huge complacent oversight that this isn't standard practice. The test readers picked up on loads of stuff. For example,
When an essential part of an explanation was missing
When I'd missed out something that people were hoping to read
When the flow didn't work properly
Innumerable confusions and ambiguities
Bits where the tone was jarring
Just as usefully, the green and red highlights allowed me to:
Know what the best bits of the book are so we can keep them as they are and write more stuff like them
Know what the worst bits are so we can cut or change them
Know what the 'meh' bits are, the bits that weren't green and weren't red, so we can improve them
For example, after the first round of test readers I noticed that a good portion of the readers were stopping half way through the book. I saw that there was a patch of about five or ten pages at this point which people weren't highlighting either green or red. They weren't bad but they were just 'meh'. It turns out people were just getting bogged down in this boring bit. I cut and changed this bit radically and in the next round of test readers, people were breezing through it with a green highlighter.
On top of all that, the test reading process has also been a really nice way to get to know people a bit better. I could talk about this test reader process all day but the next point is reminding me not to...

Short
Like everyone, I tend to write stuff that's too long (probably including this newsletter). Cutting writing is difficult because it feels like you're throwing your hard work away.
But I feel very strongly that a good clinical book should be as short as possible. A book that's as short as possible puts the reader first. It values the reader's time. In my mind, the difference between a nice short clinical book and the average textbook is the difference between these two pictures.


Of course, just because a book is short doesn't mean that once you've read it, it's done. Quite the opposite: done properly, a short book is easier to revisit over time. If you open an over-long clinical book on a random page then you're likely to see something about origins and insertions or the evidence for heel-raises or fifteen different special tests. But if you open a short clinical book on a random page then you'll read something that directly connects with a case you've just seen or a problem you've been having. A short book can have a long life.
Well, there you have it! This is what I think makes for a good clinical book, and what we’ve done to make the CES book the best clinical book it can be. It's hard to get all this stuff right, to be honest. I'm not a trained writer, and although I'm trying to learn and get better, often I aim for something and fall short. But I love this work and I hope a lot of people will love the CES book when it's finished soon.
Til next time,
Tom
For more on visual knowledge summaries, see https://www.francismiller.com/