
What we can learn from three new CES publications
(Nerve root journal club 3)

Thanks for reading the 60th edition of my newsletter. This newsletter tracks my work on lumbar nerve root syndromes aka sciatica.
Let's look at new two papers and one new book to see what we can learn about how CES presents.
Presentation, management, and outcomes of cauda equina syndrome up to one year after surgery by Woodfield et al., 2023.
For this study, Woodfield and colleagues collected data from 33 emergency spinal surgery centres across the UK, finding 621 people with discogenic CES.
How did these patients present?
Pain:
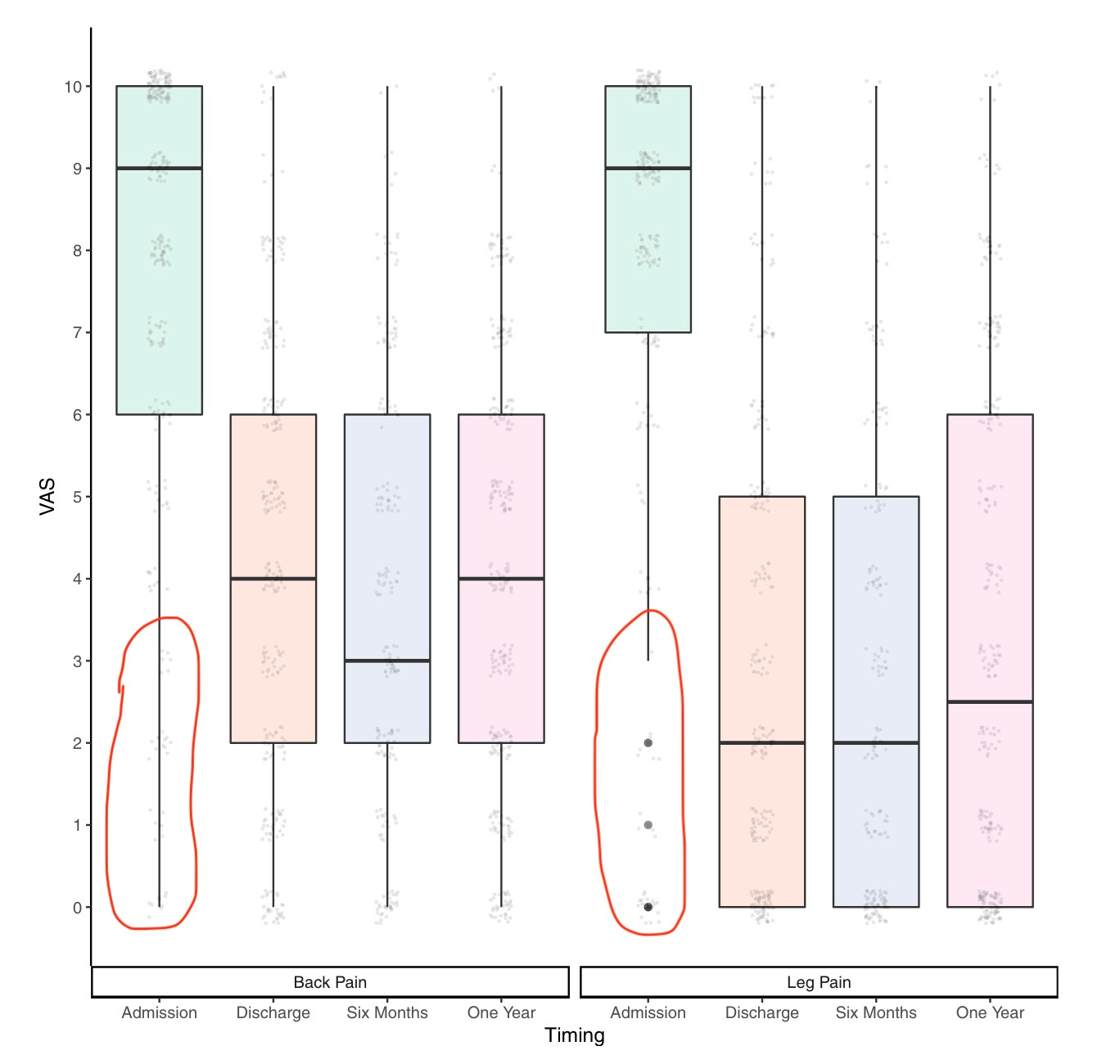
96% had back pain and 93% had sciatica. In other words, practically everybody with CES has leg pain and back pain - but not everybody! And a few people had pain that was relatively mild:
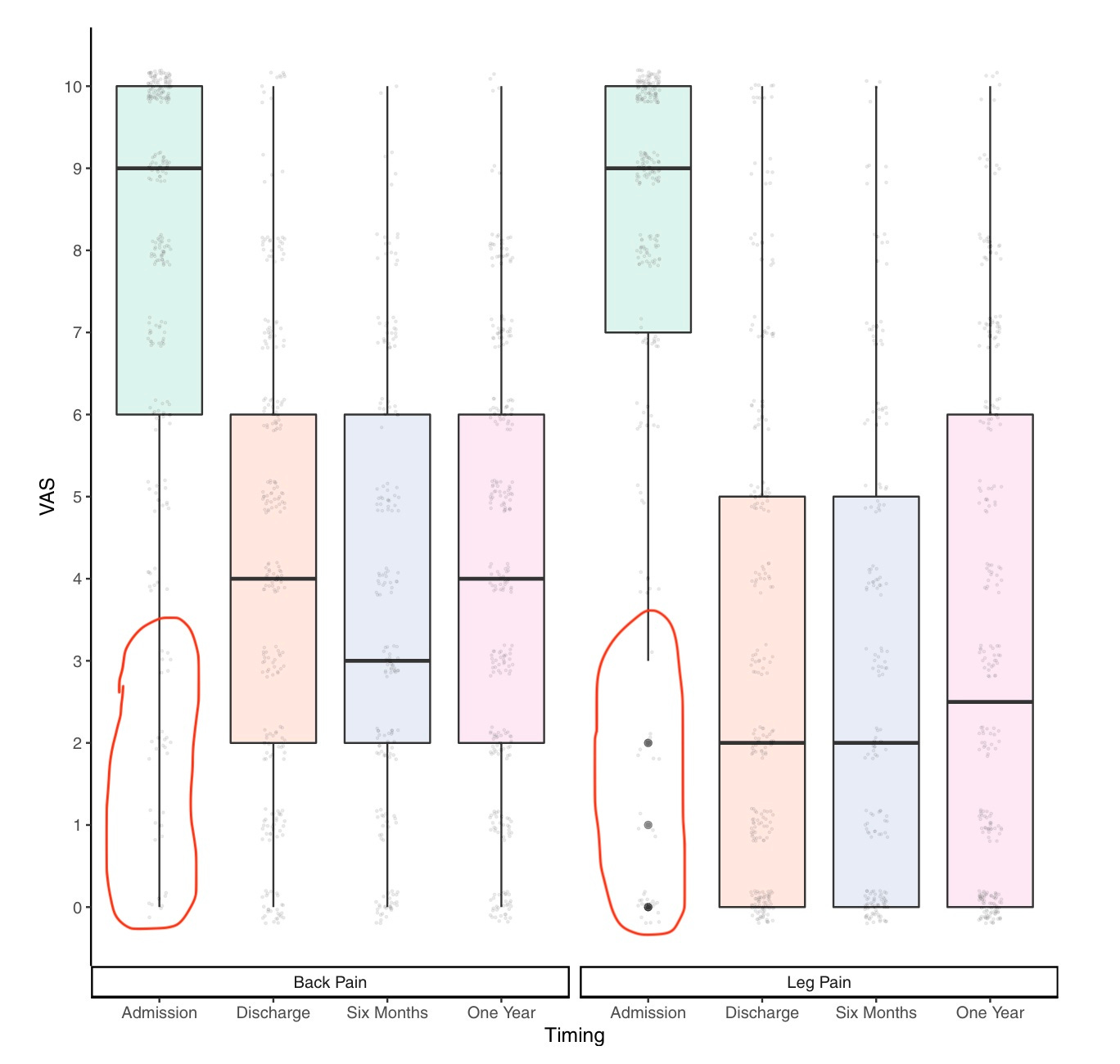
The faint grey dots in the red circles are people with CES butlittle or no leg/back pain Of all the people with sciatica, only about half of them had the red flag of bilateral sciatica. In other words, contrary to what you might expect, half of people with CES actually have unilateral sciatica.
Radiculopathy:
61% of people with CES had leg weakness and 77% had leg numbness.
As expected, radiculopathy affected the lower lumbar nerve roots more than the upper: ankle dorsiflexion and plantarflexion, L5 and S1 dermatomes, achilles reflex.
Bladder dysfunction:
83% of people had bladder dysfunction.
41% of people had retention and 40% had incontinence - we can put these people at the 'end stage' of CES, where the bladder has shut down and begun to overflow.
22% of people had altered sensation and 37% a poor stream - we can put these people in the 'incomplete' stage of CES, where the bladder is still doing something but sensory and motor function is impaired. A reminder that bladder dysfunction in CES is not just about incontinence.
Another way of looking at this is that 20% of people with CES do not have bladder dysfunction. So, just because someone doesn't have any bladder changes, doesn't mean they can’t have CES.
Loss of saddle sensation:
81% of people.
Many of these people had unilateral loss only.
Bowel dysfunction:
39% of people. Fewer than had bladder dysfunction or a loss of saddle sensation. This chimes with previous studies.
Why is bowel dysfunction less common? Partly because just use their bowel less often, so they don't notice a loss of function. On top of that, the bowel takes longer to back up and overflow than the bladder, so bowel incontinence doesn't usually occur as soon as bladder incontinence.
Sexual dysfunction:
38% of people.
In all studies like this, sexual dysfunction is the least common red flag. Why? It might be partly because sexual function is less affected than bladder function and saddle sensation. But it's also surely because most people with CES aren't trying to have sex or masturbate, and also because those that are might be reluctant to report any loss of function. And, clinicians aren't asking about it as often as they should, so it doesn’t get reported.Of people with sexual dysfunction, 63% had difficulty achieving an erection or orgasm, and 40% had a loss of sensation.
A few more notes from this study:
The average age of a person with CES was 42. This is also the average age of... people in the UK! Nevertheless, that's some evidence for the idea that CES happens in people who are young enough to still have a well-hydrated disc capable of generating the outward pressure to herniate, but old enough to have some weakening in the annular wall to allow that herniation through.
59% of people with CES were able to empty their bladder pretty well. More evidence that bladder scans are not a replacement for MRI. Sadly, it's not too reassuring when your patient is sent home from A&E because their bladder scan was normal.
The authors tried to divide CES into stages - early, suspected, incomplete and retention - but found that clinicians couldn't agree on them so they had to abandon the idea. These stages seem very useful for understanding CES on a theoretical level, and result in many a 'oh, I get it now' moment; but they don't seem that useful or reliable IRL. I believe they are being dropped from the upcoming GIRFT guidance.
The authors managed to cover every single A&E department in Scotland (!!) which meant they could reasonably assume they'd caught every case of CES in that country during the time period studied. They worked out the incidence as 2.7 cases of CES per 100,000 people per year. This confirms my suspicion that CES, though rare, is not nearly as rare as some people make out (can we stop quoting made up facts, now?)
There is much more in this fantastic study by Woodfield and colleagues, for example on the long-term outcomes of CES and the timing of surgery - but I won't go into it all here.
Determination of potential risk characteristics for cauda equina compression in emergency department patients by Angus et al., 2021.
Let's look now at another recent study by (previous podcast guest Michelle) Angus and colleagues. This was a retrospective notes review that identified 111 patients with cauda equina compression. (It's worth saying what an amazing achievement it is for the authors of this study and the previous one to get data on so many patients - even the biggest previous studies have only a few dozen patients).
What do we learn from this paper?
Firstly, when it comes to how CES presents, Angus and colleagues' results are quite similar to Woodfield and colleagues'. The age of patients was about the same, 46. Practically everyone with CES had back or leg pain, but not quite everyone. Bladder and saddle problems were the most common red flag symptoms; bowel and sexual problems, the least1.
The extra neat thing in this study is that Angus and colleagues compared all these people with CES and MRI-confirmed compression of the cauda equina to all the 888 people who came in to the emergency department suspected of having CES but who turned out to have no compression of the cauda equina on MRI2.
In other words, Angus and colleagues looked at this huge group of patients suspected of having CES, divided them into the 111 of whom did and 888 of whom didn’t, and asked… what's the difference?
Not much! For example, here is the graph comparing sensory changes in the saddle, genitals, bladder and legs. Blue = people with CES; orange = people with no CES. The bars are pretty much the same height: in patients with and without CES, the rate of sensory changes is about the same.

So too for the other red flags. Urinary incontinence, faecal incontinence, sexual dysfunction: they all occur at pretty much the same rate in people who have cauda equina compression and people who just look like they have. The same is true for the clinical tests administered in A&E, the bladder scan (again) and the digital rectal examination (which latter mirrors a recent paper by Tabrah and colleagues).
If you’d asked me before reading this study, I think I would have expected more differences than this. It’s true that in one sense you would expect CES and not-actually-CES to look similar; after all, the people with not-actually-CES have been referred to the ED because they… look like they have CES. But it’s also really quite surprising that, say, fully 31% of people with not-actually-CES have a loss of anal tone, and by contrast that only 35% of people who do have CES have a loss of anal tone.
But it’s not all null null null. There were some features that indicated someone was more likely to actually have cauda equina compression on their MRI. Those features were:
Bilateral leg pain,
Objective sensory loss (in a dermatomal distribution), and
Bilateral ankle reflex loss, especially if also bilateral knee reflex loss.
Notably these are all features of a painful radiculopathy. Maybe they filter out the people who only seem like they have CES because they are having a kind of panic or shock reaction to severe back pain, causing bladder dysfunction and functional weakness. Such people have pain and weakness but are less likely to have the particular signs and symptoms associated with an actual radiculopathy3.

In any case, Angus and colleagues are careful not to say they have discovered a special test we should all be using in clinic tomorrow - this is more information to inform further research and clinical reasoning more broadly.
The Lost Tribe, Various Authors.
So far, so many statistics. A new book written by people with CES will give us some colour. The Lost Tribe is published by the CES Champions charity. Each chapter is a different CES story, written by someone with CES.

Let’s look at a few stories from the book to see how CES might first manifest.
In one chapter, Claire explains that although she had always had grumbling back pain, the first symptom of CES was "strange sensations in my genitals". It wasn't until some time later that she had a more typical, dramatic event:
"I turned over in bed one night and suddenly this back pain gripped me, so vice-like I could hardly breathe [...] and then I became aware of pins and needles in my buttocks. It felt as if I had enormous weights strapped to each one, as if all the muscle tone had disappeared".
It's worth noting that 'pins and needles and heaviness in buttocks’ isn't explicitly a red flag for CES, although it does make perfect sense if you know how nerve root injuries work. (Another writer says "I had a horrible sense of everything drooping...")
In another chapter, Laura tells us a very different story:
"I was just sitting at my desk at work, when the toes in my left foot went numb. I shifted about and loosened my boot, thinking my footwear was just too tight [...] But that didn't help. As the morning wore on, the numbness started to spread from my big toe along to my other toes and across my foot. I took my boot off and moved my foot about to try and get the feeling back into it, as you do with pins and needles, but that didn't help either."
In another, Duncan, writes that
"One Monday morning I woke up in Bristol, and I couldn't get out of bed. I called the doctor in a panic. [After an epidural, the third in the last few years] I chose not to go home and be alone. There was something about the pain that was so unusual. I knew it wasn't right.
Luckily, my great friend Tara Palmer-Tomkinson [did I mention this is Duncan from Blue?] lived on Earls Court Road, just around the corner from the hospital, so I called her up and asked if I could stay with her for the night. [...] 'You know what you need, darling', she said in true Tara style, ‘a shot of vodka. That will sort you out.’ [...]
That night I could feel my left leg going numb, so I frantically messaged my doctor telling him this, to which he replied 'Don't worry, it's just the strength of the epidural. Give it a bit more time and everything will be fine. Tara gave me a sleeping pill to compliment the vodka and I managed to knock myself out until eight in the morning when I woke up dying for a wee. But I couldn't go. No matter how hard and how often I tried, nothing would come out.”
This book also has some very useful descriptions of red flags symptoms.
For example, here are some descriptions of bladder dysfunction:
“Like trying to pee through a straw" (Claire).
"It became more difficult to urinate. I would have to sit on the toilet and force it out" (James).
"As I was walking to the car, I was suddenly aware that I'd wet myself [...] 'What is going on?' I thought to myself" (Steven).
And some descriptions of some other red flags:
Bowel dysfunction is the "awful feeling of having a football eternally stuck up your arse", says Martin (who clearly still has the sense of rectal fullness that often goes missing with CES, despite his bowel retention).
One lady says of the sexual dysfunction that "If I shut my eyes and slept with the entire football team, I would be unaware of it".
On the pain: "I feel as if I've been dropped by a helicopter from a great height onto a telegraph pole with a pineapple strapped to the top of it". (Why do we not often talk about saddle and rectal pain with CES?)
Another thing I noticed in the book was that almost every single writer had long term back problems before developing CES. (The one exception was the writer who developed CES after giving birth, likely related to her epidural). This should put paid to the idea, that I do think is floating around out there, that CES is an acute condition that comes out of the blue and, by extension, that if someone's doesn't have CES on initial presentation then they're 'in the clear'. Disc herniations are not all-or-nothings, but ongoing events.
So keep asking, and keep educating!
This book certainly helps us to understand the importance of asking and educating patients about CES. Many of the writers describe being confused about the onset of their symptoms, not even aware that they were related to the spine, never mind something called cauda equina syndrome. "I was baffled", says one; "I couldn't explain what it was", says another. And another: "This was very weird. My left leg was completely numb and now I'd lost my ability to pee. Were the two things connected?"
In one story, James recalls that an ambulance crew came out to see him after a flare up of his long term spinal pain. They gave him gas and air and helped him get to bed, saying he didn't need to see anyone that night. "Kate [James's partner] looked doubtful, but they were medical professionals, so I didn't think to question their approach. When I woke up in the morning, the first thing I noticed was that I had wet the bed. I put it down to the fact that I was off my head on gas and air last night." James would wait another week for surgery. One senses that with just a bit more knowledge, with even just the magic words 'cauda equina syndrome', this story might have been different.
Oh, and it’s not just our patients who need to know more about CES - far from it! This book has many frustrating episodes of clinician ignorance... But let’s finish on a good note - of her GP, Claire writes,
"I owe a debt of gratitude to my own GP, Dr. White. If he hadn't taken the time to ring me at the end of his working day, to see how I was after being rebuffed at A&E, I have no doubt in my mind I would be in a wheelchair right now [...] Thank you, Dr White, I am eternally grateful."
If you take a particular interest in spinal stuff and you want to add another layer to your CES knowledge, I recommend buying The Lost Tribe (Amazon link here). There’s much more to it than what I’ve quoted, particularly around the long term story of CES and how it affects people’s lives. It’s not expensive and all the money goes to a good cause!
Wrapping up
So, three new publications, lots of new data and new stories. Thanks to the authors of these fantastic publications for all their hard work and talent.
There’s too much here to sum up neatly, but here are some final reflections:
CES has a classic picture, of back pain with painful radiculopathy plus bladder dysfunction and loss of saddle sensation. Typically, bowel and sexual dysfunction come later, if at all.
There is a lot of variation around that classic picture.
For example, no one red flag symptom must be present. Not everyone with CES has bladder dysfunction, for example, and a few people with CES people don’t even have back pain!
And, many early symptoms of CES don’t fit the classic picture. Many people with CES are not incontinent and can empty their bladder properly, but have, for example, a poor flow.
Another source of variation in CES is how individual patients experience it and describe it - after all, it’s a bio-psycho-social condition like any other.
Lots of people who don’t have CES really, really look like they do!
One implication of all this is that we should be aggressively un-learning the tick-box approach to CES and trying to develop pattern recognition about what it actually looks like, how it unfolds over time, and how patients describe it… then reasoning it through properly, educating and involving our patients as we go! (There’s a book for that 😎)
Til next time,
Tom
There were some slight differences between the two studies in how CES presents - for example, difficulty initiating urination was more common in Angus's study than full on urinary incontinence, and the rate of symptoms seemed slightly lower in general. Possibly this group of patients has been ‘caught’ slightly earlier in their CES journey?
Worth mentioning that, although it’s not cut and dry, the generally accepted definition of CES is that there must also be MRI confirmation, since the clinical signs are so nebulous. This means that people with no CE compression on their MRI technically don’t have CES, although some people prefer to call this ‘scan negative CES’, considering the fact thast the MRI probably shouldn’t be the ultimate arbiter of such things.
Supporting this, another study does find that bilateral ankle reflex loss is much less common in people with ‘scan negative CES’ (CES symptoms but no compression on MRI) than people with cauda equina compression.
this is my 16th days aster decompression surgery due to ces, idont even know what happen. there is still numbness weakness and bladder bowel and sex dysfunction. only changes in pain and light sensation on saddle area. almost giveup and hopeless. but my surgeon said its takes time.
any body here have experiences, lets we share it
I really enjoyed reading this very clear summary Tom - thank you for making research so much more accessible for us all!