
Why would sciatica take a fortnight to kick in? Pt 2.
A closer look at the nerve root.

Thanks for reading the 36th edition of my sciatica newsletter. This newsletter tracks my research as I write a book about lumbar radicular pain!
Unfortunately Substack doesn’t allow me to send really long emails. So I’ve split this piece into three; this is part two and the final installment be sent out tomorrow.
Part 1, if you missed it, is here.
Do changes in the nerve explain the delay?
It's fairly normal for nerve problems to have a delayed, sometimes very delayed onset. There are many examples. Nerve avulsion injuries can be painless until, a few days or weeks later, they definitely aren't. Apparently, for a sizable minority of amputees, it takes longer than a year for phantom limb pain to develop. Some people undergoing chemotherapy find the worst of the chemo-induced nerve pain comes weeks or months after their final dose, a phenomenon known as coasting. And nerve injuries in neonates can be painless until the child reaches puberty!
So maybe it is not just the disc. Let's look at the effects of mechanical pressure and chemical irritation on nerve roots, to see if we find a delay.
Pressure on nerves
Let's start with mechanical pressure injuries. At first, pressure might not seem like a promising explanation for a delayed radiculopathy because everyday life tells us that if you put pressure on a nerve, for example if you sit awkwardly on your leg or fall asleep on your arm, it causes a loss of strength and sensation fairly quickly (likely by depriving neurons of blood and therefore of the oxygen they need to depolarise). And animal experiments agree with this: too many studies to link to show that compressing a nerve root can cause a conduction block in the nerve within seconds.
But pressure does not always cause an immediate conduction block. There seems to be a low level of added pressure which is not enough to cause a conduction block at first, but will do so when applied for days or weeks. This was demonstrated in a study by Yoshizawa and colleagues. They applied a loose band around dogs' nerve roots, a band "slightly larger than the diameter of the root".


After one day, nothing had happened. After two weeks, still nothing had happened.
After a month, they noticed some changes that indicated the beginning of an immune-inflammatory reaction. But there was no loss of nerve function yet. After three months, Yoshizawa and colleagues found there were fewer large nerve fibers in the dogs' nerve roots, and finally observed a loss of nerve function too. After six months, fibers began to degenerate away from the site of compression (Wallerian degeneration) and loss of nerve function had become still worse.

What they had seen was a very slowly-occuring conduction block caused by a long period of slight additional pressure on a nerve root.
Many other studies support the idea that added pressure can cause nerve root damage on a timescale of weeks. For example, in a similar study to the one performed by Yoshizawa and colleagues, O’brien and colleagues found that a loose tube caused no changes in rats' nerve function until five months after application!

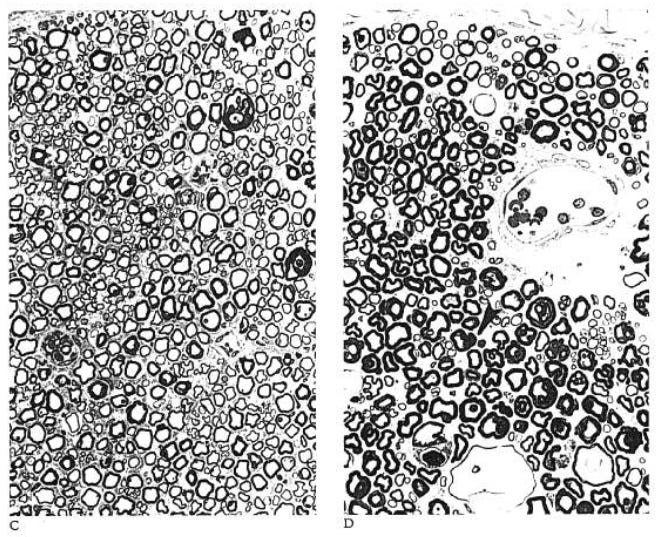
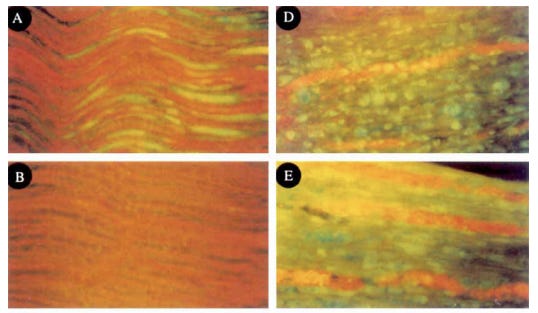
On a shorter timescale, there's also this study in which Kobayashi and colleagues observed compression-induced inflammatory changes and nerve fiber degeneration after one week (the images on the left, below) which became more advanced after three weeks (the images on the right).
Or this study, which showed that compression causes cell death of nerve root neurons that peaks at day 7, shown in the red bar here:

In fact, recent studies suggest that when the pressure added to a nerve is very slight indeed, a period of unimpaired nerve function is the norm rather than the exception!

In a way, it's really not that surprising that pressure can cause a conduction block that’s delayed by weeks or even months. After all, this is partly how things like foraminal stenosis and schwannomas (benign nerve lumps) can cause radiculopathy! Other nerve conditions like carpal tunnel syndrome come on slowly as a result of a slight increase in pressure around a nerve. I am reminded of Poulter's 'Rule of Toos': tissues are adaptable unless the stress put on them is too quick, too strong, too long (bingo) or too often.

So, we have established that, under a small amount of added pressure, a nerve can work perfectly well for a week or so but, after a while, develop a conduction block. Which sounds a lot like what happened to Adam and I. But why?
One explanation is that this small amount of added pressure is in a ‘sweet spot’: it’s enough to stop blood flowing through the nerve properly and to restrict nutrient delivery throughout the nerve, but not enough to acutely stop the nerve from doing its job of conducting action potentials. Studies in dogs and pigs support this. When 5-10mmHg of pressure is added to a nerve root, blood flow and nutritient delivery is imapired but there’s no acute loss of nerve function, even when the pressure is sustained for a few hours: the ‘sweet spot’. If that 10mmHg is applied for one week however it does eventually cause a loss of nerve function: presumably the slight impairment of blood flow and nutrient delivery finally catches up with the nerve.
I think that 'a long period of slight additional pressure' is a plausible explanation for mine and Adam's experience of a painful radiculopathy coming on a little while after a (possible) disc herniation. Certainly there is evidence that some people who end up getting surgery for painful radiculopathies have only a small amount of additional pressure on their nerve roots, at least at the time of surgery (and that in some people, removing pressure from a nerve root restores blood flow, quickly relieves pain and undoes a conduction block).
Disc material also causes delayed loss of nerve function
As I mentioned, disc herniations can injure nerve roots not only through mechanical pressure but through chemical irritation, too. The insides of a disc seem to be inherently irritating to neural tissue. And in fact, the time-scales here also seem to be in days and weeks, rather than just hours. Maybe chemical irritation by disc material explains delayed-onset radiculopathy?
End of part 2! Part 3 arrives tomorrow…
EDIT: Part 3 HERE