This is a repost from 2018, an article caled Wired Into Pain: a history of the science of pain. I hope you enjoy it. I’ve also recorded an audio version to go with it!

[2024 AUTHOR’S NOTE: I think this piece (from 2018) is still a hugely valuable introduction to the history of pain science, rich in detail. But there are some mis-steps towards the end, where it veers into a bit of a triumphalist view of recent pain science. I can’t spot much that is flat-out wrong, but I wish there were other perspectives. Don’t let that put you off reading].
I am a Physiotherapist. Almost every person I see in clinic is in pain, and most already have an idea about what has caused their pain. If they are old enough, they might say ‘overuse’, or ‘wear and tear’; if they are younger, they might say ‘bad posture’ or ‘tight muscles’; if they have had a scan, they might say a ‘slipped disc’ or a ‘bone spur’. We accept these explanations prima facie. We consider pain to be a readout on the state of the body’s tissues. Or, as one doctor wrote in 1917, it is “the unerring medical compass that serves as a guide to the pathological lesion”.
But it is only very recently that we have come to understand our aches and pains in this way. Since medieval times, until surprisingly recently, people commonly understood their pains in terms of their relationship to God, often as punishment for sin. Physical and emotional pain were entangled, along with mind, body and soul. This was the grim logic of medieval torture and self-flagellation: the truth of the soul could be accessed through the pain of the body.
But, as historian Joanna Bourke records in her book The Story of Pain, this mixture of mind, body, soul and God also allowed people to feel pain as comforting: a “vigilant sentinel […] stationed in the frail body by Providence”, as one writer put it in 1832. For others, pain was redemptive: take, for example, the early nineteenth-century labourer Joseph Townend, who resolved himself to God after undergoing surgery without anaesthetic, and reflected at the end of his life on his “sincere thanks to the Almighty God” for his agonising conversion.

Pre-modern physicians had a different perspective. Most understood pain according to humoural theory. Hippocrates and his disciple Galen considered all illness to be caused by an imbalance of the body’s humours — phlegm, yellow bile, black bile and blood — which ebb and flow in response changes in the body or its environment. This notion endured for many centuries. To one 18th century writer, pain was a consequence of “viscid blood [stopping] at every narrow passage in its progress”; to another, it was a “Nature throw[ing] a Mischief” about his body. Humoural theory is pre-scientific and seems quaint to us now. But, as Bourke points out, it accounts for an abundance of influences, from our personal temperament and our relationships to the alignment of the planets above our heads, on the pain that we feel.
Over the coming centuries, at great cost to people suffering from pain, this insight was lost. This is the story of that loss; of how we arrived at the strange, wrong idea that pain is a straightforward “guide to the pathological lesion”; and of how an emerging re-understanding of pain shows us that it is more complex and more astonishing than we have thought for centuries.
Descartes, dualism and the labelled line
“The ghost in the machine” — Gilbert Ryle

It is in the sixteenth century that we find the beginnings of the dominant modern understanding of the body and its pains. The rise of Protestantism and, amongst secular thinkers, of humanism, contributed to an increased focus on the individual and an understanding of the body as a natural, rather than a supernatural entity. Medicine became more interested in anatomy and the physical laws of nature. Vesalius published his On the Fabric of the Human Body, a compendium of illustrations of dissected cadavers based on the author’s strict, first-hand observations at a time when doctors were not accustomed to performing their own dissections. Later, physicians like William Harvey took principles from physics and astronomy to show that in many ways, our bodies can be understood as machines: pumps, pulleys and levers. Slowly, the body became less sacred and more scientific.

It was in this spirit that, in 1641, the French polymath Renes Descartes published his Meditations on First Philosophy. This work contains a drawing that became the seminal image of pain for the next three hundred years. The picture shows a kneeling boy with one foot perilously close to a small campfire. The heat of the flame sends a signal (an “animal spirit”) up a channel to the boy’s pituitary gland, which Descartes reckoned was the seat of consciousness. There, the signal elicits pain, “just as pulling one end of a cord rings the bell at the other end”.

This picture makes sense to us, it seems intuitively correct. But this is because in matters of pain we are most of us now, in the Western world at least, the children of Descartes. For pain scientists on the other hand, who have fought in recent decades to emancipate themselves from Descartes, this picture has has come to represent the original sin, the first big lie of the Western world’s understanding of pain.
It’s crimes are twofold. First, it is the essence of an idea called dualism, which holds that mind and body are separate. The body feels pain, and passes this information on to the mind. For Cartesian dualists, the body is a machine and we are a kind of ghost in the machine, receiving information about its status.
Second, the picture represents pain as being felt by a specific detector in the body, and passed up a specific pathway, the long hollow tube, to a specific location in the boy’s brain. Pain detectors, at the end of a pain pathway, that leads to a pain centre. This idea is called specificity theory, but in this post I’m going to use the term labelled line theory because although it is less common, I think it is more descriptive — a labelled line for pain.

As it happens, Descartes’ idea was more subtle than the picture and its subsequent interpretations made out. In his defence, the historians Jan Frans van Dijkhuizen and Karl A.E. Enenkel point out that Descartes knew that pain is not merely perceived, like a mariner perceives his ship, but felt, as if the mind and body are “nighly conjoin’d […] so that I and it make up one thing”. Descartes knew that we don’t just have a body; we are a body. But this subtlety was lost: the picture of the little boy with his foot in the fire has a memetic power that has carried it, along with dualism and the labelled line, through the centuries.
The nineteenth century
“Nothing less than the social transformation of Western medicine” — Daniel Goldberg
This change came gradually. It was not until the nineteenth century, two hundred years after Descartes’ Meditations, that dualism and the labelled line for pain finally established their authority in medicine.
They set in as part of a wider change in the history of medicine following the French Revolution that is sometimes now called the ‘Paris School’. The physicians of the Paris School transformed large teaching hospitals in the city to dedicate them, for the first time, to furthering scientific knowledge through rigorous observation of patients and cadavers, and the classification of disease. They explicitly rejected humoural theory, which held that illnesses are processes that are distributed around the body through the movement of viscous humours. Rather, physicians of the Paris School considered diseases to be the result of lesions localised to a single, solid organ.

Influenced by the Paris School, Victorian physicians across the Western world began to search their suffering patients’ bodies for a local, solid lesion to blame for their pain. As one New York physician wrote in 1880, “we fully agree that there can be no morbid manifestations without a change in the material structure of the organs involved”. For the first time, doctors began to think like detectives on the hunt for the smoking gun, following clues provided by the body and its sensations (it is no coincidence that Arthur Conan Doyle was a doctor before he wrote the Sherlock Holmes stories, or that he made his character Watson one, too).
This approach has tremendous diagnostic power. But, as we will see, even modern researchers find that our pain, particularly our chronic pain, resists reduction by detective work. How did Victorian physicians respond when their investigations failed to turn up a local lesion to explain pain? According to historian and medical ethicist Daniel Goldberg, many doubled down, hunting for anything they could find. As one surgeon put it, “any lesion anywhere in the body will do to account for an otherwise inexplicable pain”. And that meant any lesion: the surgeon Joseph Swann, or example, baffled by a woman’s 11-year history of pain in an apparently healthy knee, eventually attributed it to an imperfection he found, after much searching, in a nerve in her hand.

Those that could not find a lesion anywhere explained unexplained pain as one inevitably must if one subscribes to the logic of dualism: if it’s not in the body, it must be in the mind. Goldberg tells the story of the surgeon Josiah Nott who, in 1872, took on the care of an American soldier whose leg was crushed in a railway accident. The leg had already been amputated by another surgeon at a point about halfway up the calf, but the soldier had developed phantom limb pains. The original surgeon, assuming there must be a local lesion at the end of a labelled line, had then amputated the stump, but to no avail. Nott, making the same assumption, took still more from the stump the next year, and still the patient felt no relief. Later that year, Dr. Nott operated again, removing tissues from three major nerves in the shank. This pattern continued until Nott had removed the poor soldier’s leg up to four inches above the knee, and his sciatic nerve up to the pelvis. When the patient’s pain returned after this final operation, Dr. Nott reasoned that he must have acquired an addiction to opioids which was inciting him to malinger (to exaggerate or feign his disease). Nott had, horribly literally, followed the assumed cause of the disease up a labelled line through the body and, not catching it, decided it must therefore be in the mind.
This logic played out on a broad scale in physicians’ understanding of the now-forgotten condition “railway spine”, the widespread and mysterious back pain felt by the victims of train accidents. Initially, physicians thought that the trauma of a crash caused compression of nerve filaments that in turn caused pain. But as time wore on and their investigations repeatedly failed to find a tissue lesion to explain railway spine, even in cadavers, their suspicion grew that railway spine was not a ‘real’ condition at all. After all, weren’t most victims also seeking compensation from railway companies? By the beginning of the twentieth century, railway spine was known instead as “hysterical spine […] merely a psychical condition”. Dualism dictated once more that if we can’t find it in the body, it must be in the mind.

1900 to 1965
Anomalies, non-anomalies, and opening the gate
Anomalies
“[Pain] reveals only a minute proportion of illnesses and often, when it is one of their accompaniments, is misleading. On the other hand, in certain chronic cases it seems to be the entire disorder which, without it, would not exist.” — Rene Leriche, 1937
The break from Cartesianism began at the end of the nineteenth century, when the great neuroscientist Santiago Ramon y Cajal showed that our nerves, spinal cord and brain are not one thing but composed of many smaller things (which came to be called neurons) linked by gap junctions (which came to be called synapses). Decades earlier, the English neuroscientist Charles Bell had suggested that the function of the nervous system is less straightforward than the labelled line in Descartes’s picture, and Cajal’s work was proof.

As we can see by his extraordinary drawings, Cajal meticulously mapped the peripheral neurons in our arms and legs, running to the spinal cord, and the neurons running up the cord, and many of those in our brain. But, according to pain scientist and writer Fernando Cervero, the terminus for incoming peripheral neurons, the foremost part of the spinal cord that we now call the dorsal horn, was so dense and chaotic that it resisted even Cajal’s fastidious eye. He called the dorsal horn a maremagnum, a Spanish word that means ‘confused and disorganised crowd’, as in the bustle of a busy railway station. Cajal’s vision of a network of individual cells, with nodes of incomprehensible complexity, opened up the possibility that signals aren’t simply passed upwards in a linear fashion as Descartes had assumed, but are modulated along the way.
The idea that inputs to the nervous system are modulated before they ‘become’ our sensations hints at an explanation for the odd persistent pains for which Victorian physicians could find no lesion. It also begins to explain the opposite phenomenon, lesions that cause no pain, which became unignorable during the brutal first decades of the twentieth century. Doctors like Rene Leriche, on the front line in the Great War, found that soldiers with dreadful wounds often felt no pain and could undergo surgery without anaesthetic. Leriche knew this was not willpower but “certain movements of the hormones, or of the blood”, a presciently non-Cartesian thought.

During the Second World War, the American anaesthesiologist Henry Beecher built on Leriche’s observations by conducting a more methodical study at his post in Italy. He found that as many as three quarters of wounded soldiers felt little pain at the time of their injury. As one doctor put it, it was as if wounds and diseases “carry for the most part — most mercifully — their own anaesthetics with them”.


One might think that such cases would have alerted the scientific community to the fact that our nervous systems are doing something more than passively relaying pain into our brains, as labelled line theory implied. But for scientists and doctors at large, anomalies that defied labelled line went on hiding in plain sight, “discovered” periodically and then easily forgotten as they had been in the Victorian era. Phantom limb pain, for example, was unignorable during the American Civil War, and then slipped once more from popular consciousness. The doctor and writer Oliver Sacks called these periods of forgetting scotoma, dark gaps in the scientific awareness in which the prevailing theory cannot explain common phenomena and instead shoves them in the attic to think about another day. The progress of science, wrote Sacks, is faltering and haphazard, “very far from a majestic unfolding”.
Non-anomalies
“Pain is the physiological adjunct of a protective reflex” — Charles Sherrington, writing in 1900
“Pain remains a biological enigma — so much of it is useless, a mere curse” — Charles Sherrington, writing forty years later.
(Quoted in Understanding Pain by Fernando Cervero)
Rather than explaining anomalies, scientists studying pain at the beginning of the twentieth century focused on a series of discoveries that appeared, at first, to confirm labelled line theory. The British neuroscientist Charles Sherrington had coined the term “nociceptor” for the neurons that convey danger messages (elicited by things like heat, intense mechanical pressure or an incision to the skin) to the brain, and in the following decades researchers slowly but successfully identified and isolated these cells.
Starting in 1912, American scientists performed the first anterolateral cordotomy, slicing through the part of the spinal cord that was theorized to carry danger messages to the brain and appearing to stop pain in its tracks. Later, the success of such operations would prove to be temporary, but the procedure did show that this part of the spinal cord houses Sherrington’s nociceptors. In 1927, the Americans Herbert Gasser and Joseph Erlanger established that different nerve fibers conduct signals at different velocities, and classified them according to their diameter as A, B and C fibers. A fibers were widest and conducted signals the quickest; C fibers were the most narrow and slow. They found that one sub-type of A fibers, A-delta fibers, conducted the relatively quick sensation of dull pain we feel when we stub our toe; and that C fibers conduct the slower, stinging pain that arrives later. Again, this neat distinction would later prove to be more complicated, but the discovery was further evidence for a labelled line of pain. Gasser and Erlanger were only able to look at conduction signals from a whole bundle of nerves and so it was not until 1958 that Ainsley Iggo was first to record individual A-delta and C fibers and isolate Sherrington’s nociceptors for the first time.

Opening the gate
“It may seem easy, but it was not” — Ronald Melzack
Despite this series of discoveries in favour of labelled line, some researchers could not shake from their minds those confounding anomalies: pain without lesion, and lesion without pain. And so, at last, the science of pain began to wake from its scotoma. Some scientists began to propose a theory to compete with labelled line called pattern theory, which held that it is not the stimulation of specific nerves that causes the sensation of pain, but that the way in which nerves are stimulated, spatially and temporally. Pattern theory was vague, and had nowhere near the amount of evidence that supported labelled line theory, but it did hint at an answer to some of the anomalies that had been documented in the recent scientific literature, such as the way pain spreads beyond the site of an injury and the way rubbing a pain can make it temporarily feel better. Pattern theory was taken up in Oxford in the 1940s and 50s, where the brilliant British neuroscientist Pat Wall was beginning to develop ideas he would turn into gate control theory, a whole new model of pain.
In 1959, Wall moved from Oxford to the Massachusetts Institute of Technology where he met Ronald Melzack. Melzack, a Canadian, had just arrived at M.I.T. to take up a post as assistant professor of Psychology, and found to his annoyance that he could not perform research on animals in the university’s Psychology building. So, Melzack decamped to Wall’s lab. The two quickly took up a discussion on the inadequacy of Cartesianism and decided to come up with a new theory to “entice spinal-cord physiologists away from [labelled line]”.
From his previous research, Melzack knew the brain sends messages down the spinal cord to inhibit the messages coming up it, exerting a kind of ‘top-down’ control on incoming information. From his own experiments, inspired by pattern theory, Wall knew that different inputs into the nervous system are weighed against each other somehow in the spinal cord, competing to be ‘sent up’ to the brain. Despite their discussions, Melzack and Wall’s ideas remained inchoate until, in 1962, Melzack stumbled on the Dutchman Willem Noordenbos’s pattern-theory hypothesis that large A-fibers carrying touch signals might somehow inhibit small C-fibers carrying danger signals.
Melzack calls this moment a “flash of insight”. Noordenbos had theorized that this modulation happened in the substantia gelatinosa, which is part of the terminus for incoming information at the spinal cord. Wall knew that large fibers and small fibers entered the substantia gelatinosa at opposite ends, and theorised that it was this setup that allowed the one to inhibit the other, like closing a figurative ‘gate’. The weight of signals from large and small fibers would determine what kind of message was allowed up to the brain.


In 1963, Melzack moved to McGill University in Canada, but travelled South over the border when he could to visit Wall’s home in Boston where, over large amounts of duty free whiskey, the two put the finishing, definitive touches to their work. Their theory differed critically from Noordenbos’ because they proposed that the brain itself plays a role in processing at the substantia gelatinosa, by sending signals down the spinal cord to make the ‘gate’ more likely to open or close to danger signals. This was gate control theory.

For the first time, science had a model that began to explain pain anomalies. According to gate control theory, for example, the brain of a soldier who has sustained an injury can send messages down the spinal cord to close the gate to incoming danger signals. Over fifty years have passed, and gate control theory has turned out to be wrong in lots of little ways, but right in one big way: it is modulation in the spinal cord and the brain, or the central nervous system, that explains why pain is so rarely the reliable sign of tissue status that Victorian scientists assumed it was.

Neuromatrix theory
“We need to go… to the brain” — Ronald Melzack
“When you feel a pain in the leg that has been amputated, where is the pain? If you say it is in your head, would it be in your head if your leg had not been amputated? If you say yes, then what reason have you for ever thinking you have a leg?” — Bertrand Russell
Gate control theory was a great advance but Melzack and Wall knew their theory was incomplete. According to Oliver Sacks, it is by studying anomalies — phenomena not explained by the prevailing theory — that researchers wake from scotoma and begin revolutions in scientific understanding. So it was that Melzack’s interest in the anomaly of phantom limb pain led to neuromatrix theory, the next great boost that finally allowed pain science to escape to orbit of Cartesianism
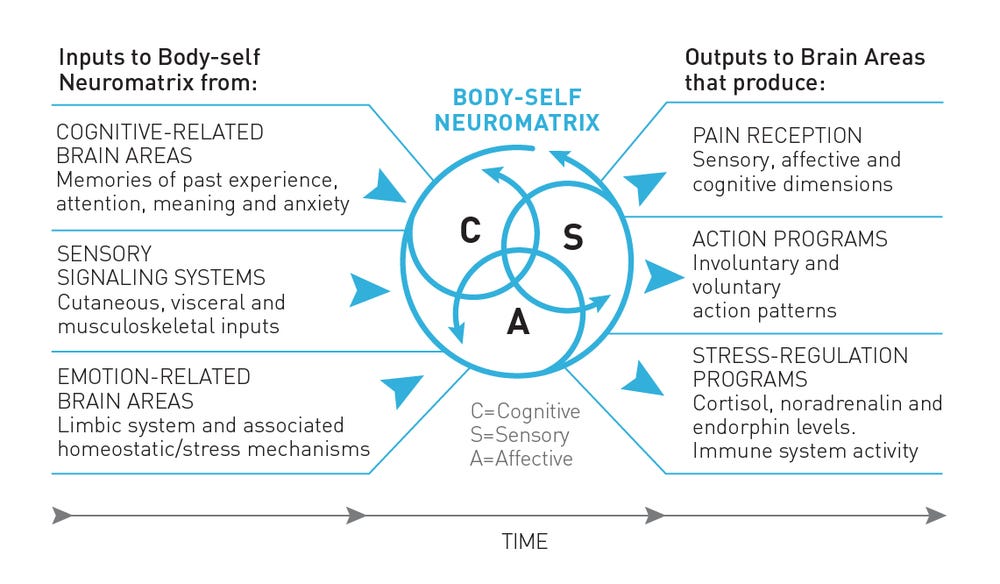
If people without limbs have phantom pain, Melzack reasoned, it follows that the origins of the pattern of pain lie not in the limb but in the brain. And not only pain, but the sensation of having a body in its entirety — its place in the world, its shape, its movements — is housed, in what Melzack came to understand as a series of loops and patterns of neurons, inside our brains. This brain architecture is the neuromatrix.
Incoming information, then, is not what holds the essence of our sensations; it merely triggers the neuromatrix, already inscribed in the brain, to ‘produce’ the sensations we feel. If a boy puts his foot in a fire, the nerves do not tell a passive brain “here is pain”; the nerves simply say “here is an intense input”, and the neuromatrix does the rest.
How do we get a neuromatrix? Melzack says it is inborn, but then shaped by experiences. So, your neuromatrix develops your own personal signatures for familiar pains, like the pain you might feel in your back when you bend. Crucially, the neuromatrix uses our thoughts and emotions to generate our sensations, as well as sensory information. This makes sense: think of a stroke on the leg from your partner and one from an unappealing stranger. The same sensory input feels different.
So, if you believe the cause of your back pain is something threatening, like a suspected spinal cancer or a ‘slipped’ disc, it willfeelworse than if you believe it is something benign, like a muscle strain. If a conscripted soldier sustains a battlefield injury that means he will likely have to leave the trenches to convalesce behind the front lines, that wound may not feel as bad as it would for a factory worker, for whom it could mean a loss of livelihood. If you have just been made redundant, or become divorced, than the incoming danger signals from an incipiently arthritic hip might suddenly start triggering your neuromatrix to produce a deep aching pain in your joints.
Pain is intimately integrated with meaning, and informed by the broader context of our lives. And there is no labelled line: pain is the output of a widely-distributed neural process that takes input from countless biological, psychological and social factors.
The sensitive nervous system
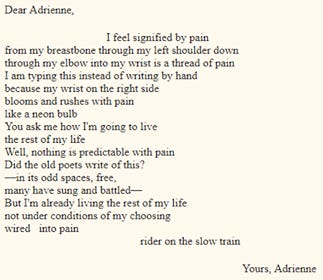
“Not under conditions of my choosing / Wired into pain / Rider on the slow train” — Adrienne Rich
Researchers have used the neuromatrix as a foundation to develop our understanding of pain. For example, towards the end of the 1970s, scientists began to establish that the endings of our danger messenger neurons, the ones Sherrington christened nociceptors, become more sensitive the more they are used, a process called peripheral sensitization. But perhaps the most remarkable development since Melzack proposed the neuromatrix was Clifford Woolf’s discovery of central sensitization.
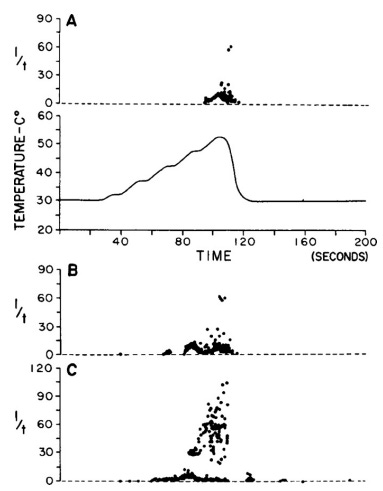
On completing his medical training in South Africa in the early 1980s, Clifford Woolf joined Pat Wall’s laboratory in London. He was not content with measuring the readouts from individual chains of neurons, and instead began to monitor broader bursts of activity which he thought would give him more insight into the pain system as a whole. He started to measure the output of the neurons that cause muscles to flex away from a dangerous stimulus (think of touching a hot stove and retracting your hand before you are even conscious of pain). Investigating on rats, he found that most of these cells responded to dangerous stimuli, such as heat and pinch, in a fairly narrow field — say, one toe. But, some cells had a very wide receptive field and would respond to even light, non-dangerous touch. Why would rats have neurons designed to elicit a withdrawal response to light touch?
It took Woolf some months to realise that he was only finding these neurons at the end of the workday, when his rats had already been subjected to hours of pain-inducing stimuli. He calls this his “eureka moment”. He had not discovered that rats have certain neurons that are super sensitive across a wide receptive field: he had discovered that a rat’s nervous system becomes super sensitive across a wide receptive field when it has been exposed to prolonged danger. Woolf had discovered an ‘amplifier’ mechanism in the spinal cord. This phenomenon is central sensitization.
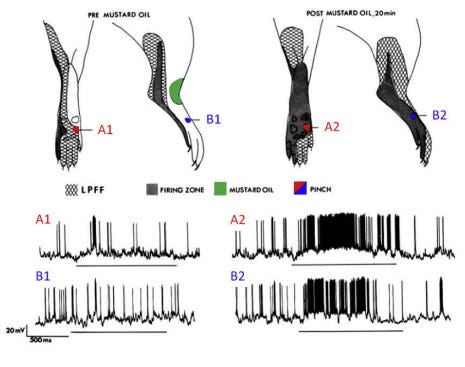
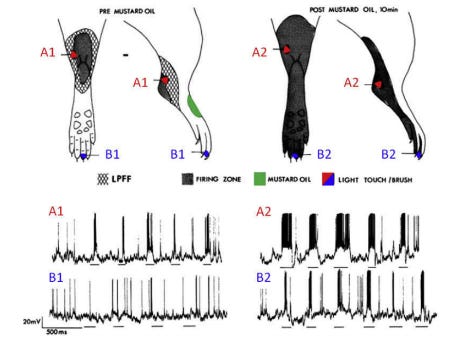
Woolf was the first person to show that the nervous system is not hard-wired for pain but plastic. Prolonged nociception can change the behaviour and the architecture of the nervous system so that non-dangerous inputs (like light touch) are felt as painful, and dangerous inputs (like a pinprick) produce more pain than they otherwise would have done. To top it off, this whole pain experience also spreads beyond the original site of injury. The great physiotherapist Louis Gifford described central sensitization as like tapping X on your computer keyboard three times, and 10 X’s of different sizes and colours popping up on the screen.

A mild and benign form of central sensitization is common and almost immediate after most injuries — after you burn your hand or sprain your ankle, it is your body’s way of protecting itself. But central sensitization can wear on and, in many cases, persist and get worse long after any injury has healed. If you or someone you know has widespread back pain that flares up with the slightest movement, or has osteoarthritis in their hip that seems to spread all the way down their leg, they might have central sensitization.

Central sensitization can affect many different functions, not just pain. People with ongoing, maladaptive central sensitization can be tense and forgetful, and sensitive to bright lights, loud noises and chemicals. It is also a feature of irritable bowel syndrome, migraine and chronic fatigue syndrome, and often goes hand in hand with anxiety and depression.
So long, labelled line: Grappling with complexity
“Pain cannot easily be divided from the emotions surrounding it. Apprehension sharpens it, hopelessness intensifies it, loneliness protracts it by making hours seem like days. The worst pain is unexplained pain” — Hilary Mantel
“The basic idea of pain modulation implies that the output can be different to the input at every stage in the transmission of pain signals throughout the brain” — Fernando Cervero
Central sensitization is just one discovery that has enhanced our understanding of pain. There are many more examples. Descending modulation is the ongoing process by which the brain sends signals down the spinal cord to simultaneously inhibit and facilitate incoming danger signals, a mechanism Leriche anticipated when he observed that battlefield wounds “carry […] their own anaesthetics with them”. In people with persistent pain, descending modulation may be set for a net facilitation of incoming danger messages. Researchers have also expanded our understanding to include the immune system, which aids and abets the nervous system as it produces pain. They have found out that nociceptors, far from lying waiting for an intense stimulus as Sherrington imagined, are actually firing regularly throughout the day, every time we use a pair of scissors, ride a bike or go on a long walk, without (if we are lucky) our neuromatrix producing the experience of pain. Conversely, clever experiments have shown that nociception is not even necessary for pain, giving credence to the stories of people who narrowly escape injury but, believing they have been hurt, writhe in agony. And, we know that stress, even the stress of early life events, plays a vital role in ongoing pain, and that our stress system and pain production system are intimately linked.

The contrast between the byzantine, distributed complexity of the mechanisms of pain and the singular experience of pain — I feel it here — is remarkable. Scientists have made various attempts to simplify the mechanisms into something more understandable and more useful to lay people. The neuroscientist VS Ramachandran has said that “pain is an opinion on the organism’s state of health rather than a mere reflective response to an injury”, a stark contrast to the old-fashioned idea of pain as “the unerring medical compass that serves as a guide to the pathological lesion”.
The scientists and physiotherapists Dave Butler and Lorimer Moseley put it elegantly:
“We will experience pain when our credible evidence of danger related to our body is greater than our credible evidence of safety related to our body. Equally we won’t have pain when our credible evidence of safety is greater than our credible evidence of danger.”
In other words, pain is not measuring damage, it is a protective strategy, just one of many (along with local and systemic inflammation, changes in movement like tensing or bracing, the feeling of stiffness, and so on) that the body enacts in response to credible evidence of danger.

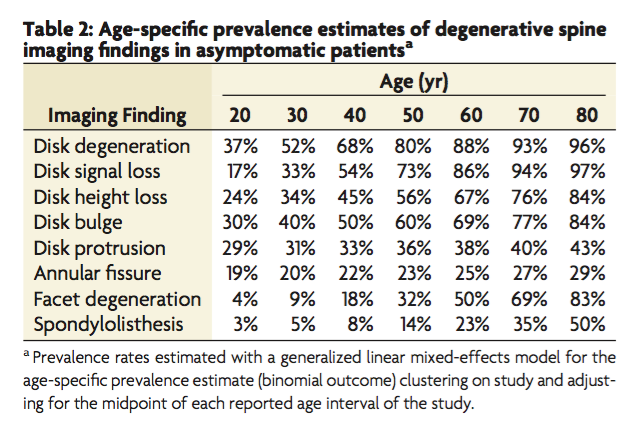
This evidence of danger often includes nociception (signals from tissue damage), but the neuromatrix uses many other sources, too. For example, if someone has back pain and a doctor tells you your x-ray shows “wear and tear” or “degeneration” in your spine, they have received a clear message of danger related to your body that is likely to make their pain worse. Indeed, people with back pain who get an MRI actually reduce their chances of recovery. On the other hand, if that person’s doctor (or physiotherapist!) tells them that the findings on their scan are normal age-related changes (or, better yet, doesn’t order a scan at all), that is a clear safety message. Safety messages can come from anywhere. Exercise can send safety messages to your neuromatrix, and so can a supportive workplace or having a friend around to talk to.
Reflections
Slow progress, hopes for the future and a note of caution
Slow progress
“I am still not happy with what has been accepted” — Pat Wall, 1999
Danger sharpens pain; safety soothes it. Why, then, do health professionals continue to give people with persistent pain credible evidence of danger? Apart from the obvious — that there is money in telling people their spines are crumbling and their pelvises are out of line, that they have muscle knots that need releasing and cores that need stabilizing — it is because, just as Descartes’ model of pain took almost three centuries to reach its zenith in Western culture, the neuromatrix, still only forty years old, has been accepted only falteringly even in medical circles, and hardly at all in the wider culture.

Indeed, in many ways the twentieth century has doubled down on labelled line. Take, for example, the dominance of the orthopaedic understanding of low back pain, which the late Scottish doctor and historian Gordon Waddell called “the dynasty of the disc”. Waddell traces the tenuous association of the lumbar disc with low back pain to a fateful cluster of papers published at the beginning of the century by orthopods searching, like Victorian physicians had done before them, for a pot of gold at the (wrong) end of the labelled line. Even today, routine orthopaedic surgeries like lumbar fusion, knee arthroscopy and shoulder decompression are amongst the most low-value, least evidence-based treatments in healthcare, still performed largely because of inertia and unexamined Cartesianism.
Many physiotherapists practice with the same habits. Like Joseph Swann, we might conduct a questionable root-cause analysis up or down a kinetic chain to find an ‘issue in the tissues’, settling on a pronated foot, a slumped posture or a valgus (in-falling) knee. Like Josiah Nott, when a patient has failed a course of ‘corrective’ exercise to ‘fix’ their body we might decide their problem is primarily ‘psycho-social’, a euphemism for in-their-mind. This is understandable, it takes great effort to shift from Cartesianism to the neuromatrix; I have been trying for years and I am still astonished when a new study is published showing, for example, that there are no major physical risk factors for a first episode of neck pain, but multiple psychological ones, like depression, and social ones, like role conflict. Still, it is imperative that medical professionals of all stripes challenge their colleagues who promote themselves as experts but who practice with unreconstructed Cartesianism.
Hopes for the Future
“While pain sufferers do not have the luxury of denying the reality of their pain, they can and do deny its legitimacy, thereby internalising the stigma so frequently directed at people in pain.” — Daniel Goldberg
The neuromatrix model has the potential to be immensely liberating for patients. For people with everyday predicaments of life like the back or shoulder pain we all get from time to time, there is the reassuring message that pain is not an indicator of damage and they are safe to move. In fact, movement, as opposed to protecting the painful joint, is the way to go in the long run. For people with more profound, widespread and recalcitrant pain, understanding why their pain is the way it is can help with the process of acceptance, and knowing pain is multifactorial can open up new therapeutic options to help calm down a sensitive nervous system.
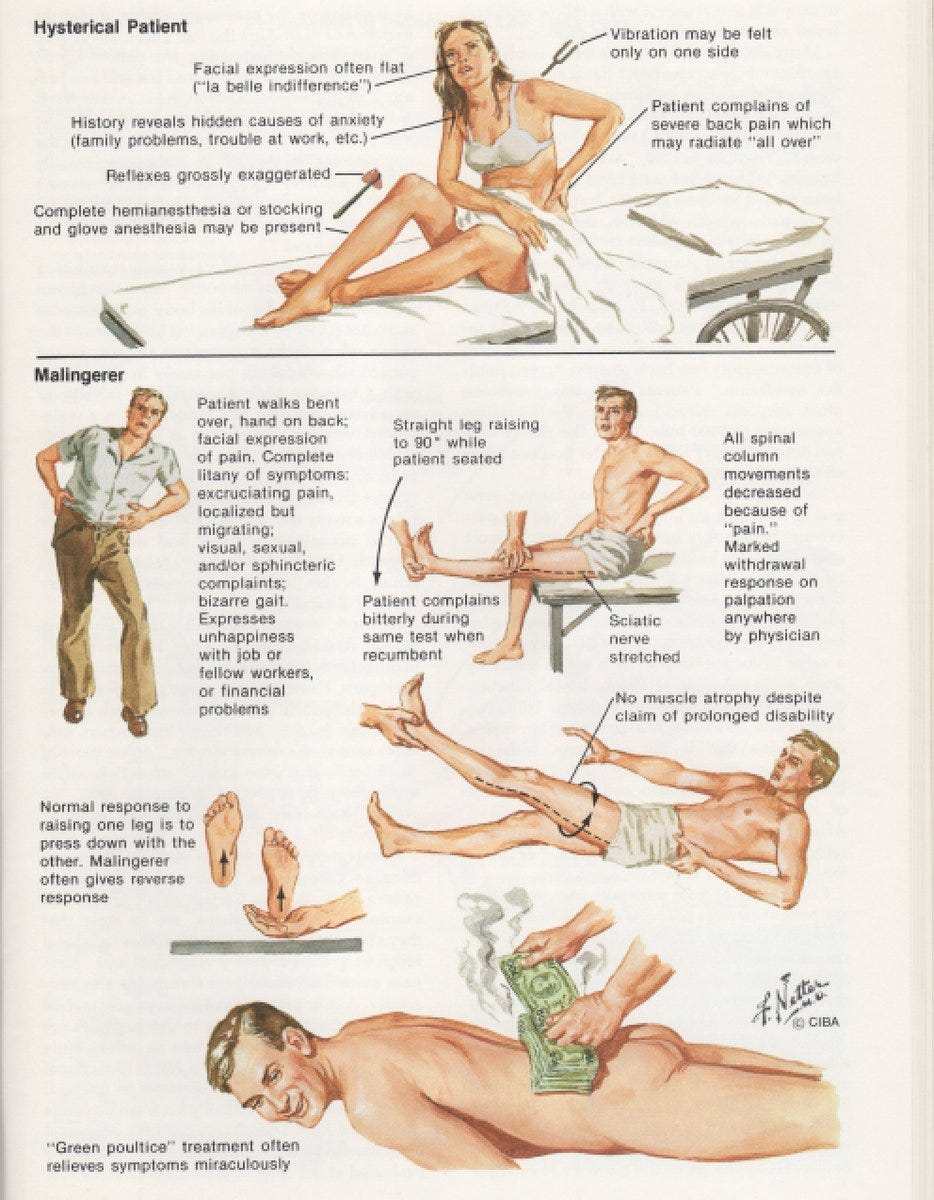
The neuromatrix could also militate against the way Cartesian thinking drives stigmatization of people with chronic pain. Cartesian dualism casts pain as a two-step sequence of events: the body senses pain, then the mind reacts. As recently as the 1980s, words like “hysterical” or “psychogenic” were used to describe people who appeared to be ‘over-reacting’ to their pain. It is this thinking that allows us to sort people into those who are responding appropriately to their pain, and those who are ‘being dramatic’. The saddest effect of this stigma is when patients internalise it, believing that they are not ‘coping’ properly with ‘a bit of back pain’.
So patients and health professionals need to know that dualism is bogus: as Pat Wall himself put it, “the separation of sensation from perception was quite artificial… sensory and cognitive mechanisms operate as a whole”. Or, in the words of neuroscientist Fernando Cervero, “emotional, sensory and cognitive elements aren’t organised in a hierarchical way, but in a cooperative way […] interacting to generate the final pain experience”.
A note of caution
“Nineteenth century physicians drain[ed] pain of any intrinsic meaning altogether, making it little more than a sign or symptom of something else” — Joanna Burke
“[The challenge is] to allow a rapprochement between the world of the clinician and the world of the person in pain” — Quinter et. al (2008).
The neuromatrix and all its attendant discoveries have revolutionised how medical and health professionals should approach people in pain. It is a rare true paradigm shift. But there is danger in complacency. “Now is not a time for professional hubris or the proclamation of truth by a few”, warn the rheumatologists John Quintner and Milton Cohen. The battle to understand pain is only half won. It is all too easy to be drawn back into the orbit of dualism, not only between the mind and body, but between the clinician and the patient, or the researcher and the sufferer. Centuries-old habits die hard, and we have long made the person-in-pain an object of enquiry. But this can only take us so far; as Quinter and Cohen assert, “the pain of another person is irreducible to its neuronal correlates”. We can only really know pain through dialogue.
It is difficult to talk properly about pain. Being in deep pain can be a harrowing, abject, solitary experience. And apart from anything else, often we just don’t have the words: Virginia Woolf, no stranger to pain, lamented that English has a rich vocabulary for love, but a meagre one for pain. The poet Emily Dickinson said that pain “has an element of blank”.
But it can be done. Joletta Belton, a blogger with persistent pain, recently tweeted about the two clinicians who had helped her the most. “It wasn’t just their words” she wrote, “it was that they listened first. And understood. Listening matters […] I wasn’t interrupted or lectured, they didn’t try to ‘educate’ me or alter my narrative to suit their own […] I felt what I said was of value. I felt human, of worth. That’s invaluable.”
It may seem strange to end a post about science with a note on the importance of listening, but in the context of the neuromatrix it makes perfect sense. Listening to people in pain is what’s needed to undo the damage that has been done, and take the progress that’s been made to the next level.
Belton’s experience echoes a vignette reported by Joanna Bourke in The Story of Pain.During a medical consultation in 1730, an embarrassed patient found himself apologising to his physician for boring him with “so tedious a Tale”. The patient’s physician protested: “Your Story is so diverting, that I take abundance of delight in it, and your Ingenious way of telling it, gives me a greater insight into your distemper, than you imagine. Wherefore, let me beg of you to go on, Sir: I am all attention, and shall not interrupt you.”
Selected bibliography
Journal Articles
Allan, D. and Waddell, G. (1989). An historical perspective on low back pain and disability. Acta Orthopaedica Scandinavica, 60(sup234), pp.1–23.
Arnaudo, E. (2017). Pain and dualism: Which dualism?. Journal of Evaluation in Clinical Practice, 23(5), pp.1081–1086.
Baliki, M. and Apkarian, A. (2015). Nociception, pain, negative moods, and behavior selection. Neuron, 87(3), pp.474–491.
Bourke, J. (2014). Pain sensitivity: an unnatural history from 1800 to 1965. Journal of Medical Humanities, 35(3), pp.301–319.
Brodal, P. (2017). A neurobiologist’s attempt to understand persistent pain. Scandinavian Journal of Pain, 15(1).
Cohen, M., Quintner, J., Buchanan, D., Nielsen, M. and Guy, L. (2011). Stigmatization of Patients with Chronic Pain: The Extinction of Empathy. Pain Medicine, 12(11), pp.1637–1643.
Chapman, C., Tuckett, R. and Song, C. (2008). Pain and stress in a systems perspective: reciprocal neural, endocrine, and immune interactions. The Journal of Pain, 9(2), pp.122–145.
Eriksen, T., Kerry, R., Mumford, S., Lie, S. and Anjum, R. (2013). At the borders of medical reasoning: aetiological and ontological challenges of medically unexplained symptoms. Philosophy, Ethics, and Humanities in Medicine, 8(1), p.11.
Goldberg, D. (2012). Pain without lesion: debate among American neurologists, 1850–1900. 19: Interdisciplinary Studies in the Long Nineteenth Century, 0(15).
Goldberg, D. (2017). Pain, objectivity and history: understanding pain stigma. Medical Humanities, 43(4), pp.238–243.
Iannetti, G. and Mouraux, A. (2010). From the neuromatrix to the pain matrix (and back). Experimental Brain Research, 205(1), pp.1–12.
Kerry, R., Maddocks, M. and Mumford, S. (2008). Philosophy of science and physiotherapy: An insight into practice. Physiotherapy Theory and Practice, 24(6), pp.397–407.
Latremoliere, A. and Woolf, C. (2009). Central sensitization: A generator of pain hypersensitivity by central neural plasticity. The Journal of Pain, 10(9), pp.895–926.
Melzack, R. (1999). From the gate to the neuromatrix. Pain, 82, pp.S121-S126.
Melzack, R. (2005). Evolution of the neuromatrix theory of Pain. The Prithvi Raj Lecture: Presented at the Third World Congress of World Institute of Pain, Barcelona 2004. Pain Practice, 5(2), pp.85–94.
Melzack, R. and Katz, J. (2012). Pain. Wiley Interdisciplinary Reviews: Cognitive Science, 4(1), pp.1–15.
Mendell, L. (2014). Constructing and deconstructing the gate theory of pain. Pain, 155(2), pp.210–216.
Moayedi, M. and Davis, K. (2013). Theories of pain: from specificity to gate control. Journal of Neurophysiology, 109(1), pp.5–12.
Moseley, G. and Butler, D. (2015). Fifteen years of explaining pain: the past, present, and future. The Journal of Pain, 16(9), pp.807–813.
Moseley, G. (2007). Reconceptualising pain according to modern pain science. Physical Therapy Reviews, 12(3), pp.169–178.
Neilson, S. (2015). Pain as metaphor: metaphor and medicine. Medical Humanities, 42(1), pp.3–10.
O’Sullivan, P., Caneiro, J., O’Keeffe, M. and O’Sullivan, K. (2016). Unraveling the complexity of low back pain. Journal of Orthopaedic & Sports Physical Therapy, 46(11), pp.932–937.
Perl, E. (2007). Ideas about pain, a historical view. Nature Reviews Neuroscience, 8(1), pp.71–80.
Quintner, J., Cohen, M., Buchanan, D., Katz, J. and Williamson, O. (2008). Pain Medicine and Its Models: Helping or Hindering?. Pain Medicine, 9(7), pp.824–834.
Thacker, M. and Moseley, G. (2012). First-person neuroscience and the understanding of pain. The Medical Journal of Australia, 196(6), pp.410–411.
Wiech, K. (2016). Deconstructing the sensation of pain: The influence of cognitive processes on pain perception. Science, 354(6312), pp.584–587.
Woolf, C. (2007). Central sensitization. Anesthesiology, 106(4), pp.864–867.
Books
Cervero, F. (2014). Understanding pain. Boston: Mit Press.
Butler, D. and Moseley, G. (2015). Explain pain. Adelaide: Noigroup Publications.
Bourke, J. (2014). The story of pain. Oxford: Oxford Univ. Press.
Moseley, G. and Butler, D. (2017). Explain pain supercharged. Adelaide: Noigroup Publications.
Blog posts
Pain is weird by Paul Ingraham
Pain really is in the mind, but not in the way you think by Lorimer Moseley
Central sensitization in chronic pain by Paul Ingraham
My own chronic pain story by Paul Ingraham
Easing musculoskeletal pain Information leaflet
Tell me your story by Joletta Belton
Podcasts and lectures
The Pain Revolution by Lorimer Moseley
Pain: past, present and future with Mick Thacker
Understanding Pain in 2025 by Mick Thacker