


Four to six schmeeks.
How long does sciatica last?

“How long’s it going to take to get better?”
Well, the NHS website says:
“Sciatica usually gets better in 4 to 6 weeks”
Spine Health says that sciatica
“May flare intermittently or remain constant for up to 4 to 6 weeks”
According to StatPearls,
“Most cases of sciatica resolve in less than 4 to 6 weeks”
And the British Associaton of Spine Surgeons has this graph, which says that after 4 weeks, nearly 80% of people are no longer complaining of pain1:

Hmmm….!
What does the research say? Well, in this post I’ll lay out some broad conclusions2. And at the end, we’ll come back to the ‘4-6 weeks’ line to see how it holds up!
First conclusion:
There’s a rule of thirds for acute sciatica.
For people with very acute sciatica, there's a rule of thirds: Over the next couple of weeks, you have about a 1 in 3 chance of your pain greatly improving; a 1 in 3 chance of it improving a fair amount; and a 1 in 3 chance of it staying the same or getting worse.
The main source for this conclusion is a study by Vroomen and colleagues, which is one of the few studies that catches people very early after the onset of their pain and follows up in the short term. What did it find? Amongst 183 people with an average of two weeks of lumbar radicular pain, 65-70% said they experienced "any improvement", whether a little or a lot, after two weeks. And 35-37% of them said they were greatly improved. Average improvement was gradual over the two weeks:

We can cross-check the study by Vroomen et al. against an older study by Hakelius, which looked at 447 patients with an acute onset3 of radicular pain and found a very similar pattern of improvement4. It’s worth also mentioning a study by Weber and colleagues, who followed 208 patients with acute radiculopathy and also observed a significant improvement in the first four weeks, in this case measured in mean pain scores:
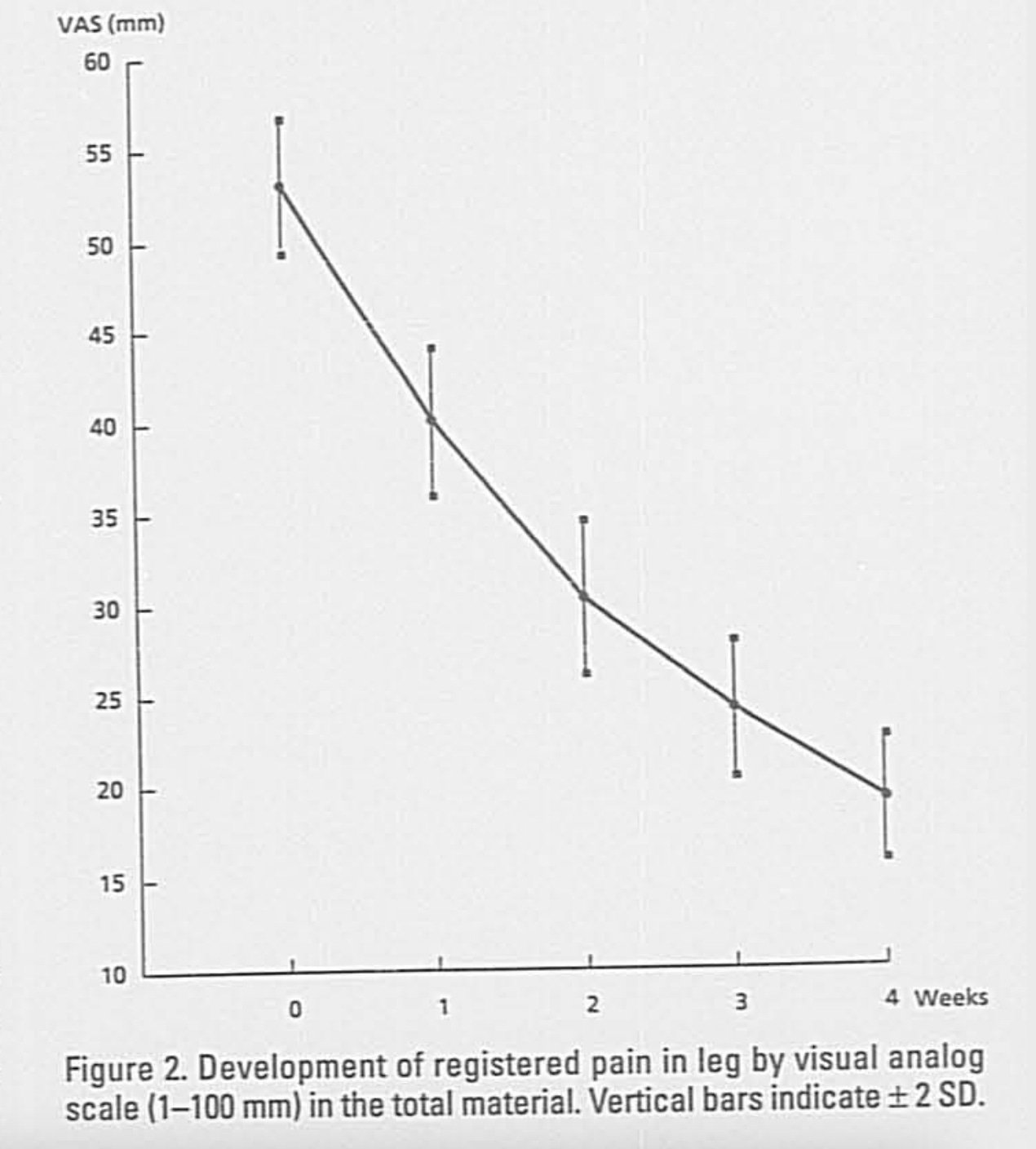
Both these studies back up the results from the paper by Vroomen et al. and increase my confidence in a rough ‘rule of thirds’.
Surprisingly, that’s about all the research we have on the very acute phase. What about when we extend the timescale a bit?
There’s a 50% resolution rate within three months.
For about half of all people seeking care with sciatica, pain will resolve, or nearly resolve, within three months.
There are two high-quality, landmark RCTs that find strikingly similar results about when people first feel like their pain has resolved.
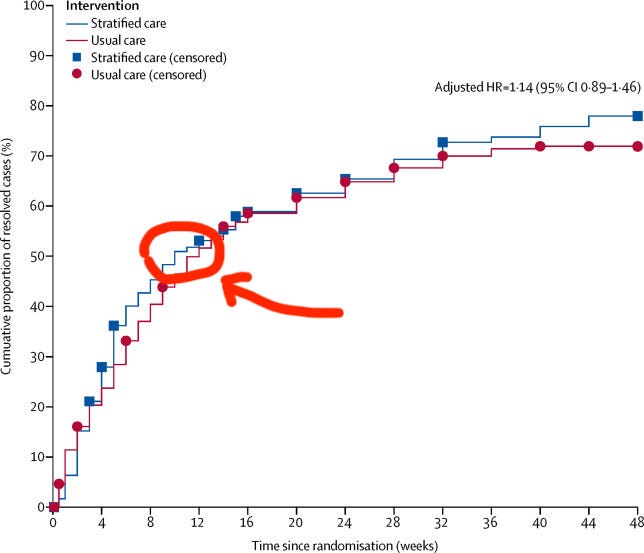
The first, the recent SCOPIC trial, enrolled a group with a mixture of acute, subacute and chronic sciatica. (Specifically, the group had had sciatica for an average of two months, with about half the group having pain for more than three months.) After three months of mostly conservative treatment, 50% of the group described themselves as recovered:
The other high-quality RCT is by Peul and colleagues also enrolled people with an average of two months of sciatica, and also found that after 12 weeks, 50% of them described themselves as recovered.

To those two trials, we can also add the previously-mentioned older study by Hakelius, which found that 50% of people were free of symptoms in just two months5
Now, to be clear, this isn’t really natural history any more. Most of these people aren’t being followed from the time of the onset of their sciatica, and they’re also all receiving treatment. Rather than natural history, this is the ‘clinical course’ of sciatica - in other words, ‘what’s probably going to happen from the time of your first appointment on, irrespective of how long your pain has been going on’. It’s not nearly as useful as true natural history, but it’s what we’ve got.6
In any case, it looks like half of all patients with sciatica recover within three months. Or, to put it another way, when you see a new patient with sciatica, there’s a 50/50 chance their pain will be gone or essentially gone in the next three months. And that goes for all patients, whether acute or chronic - but we can assume people with acute pain will have better odds.
The problem, as we’ll see soon, is that once pain has resolved… it might not stay resolved.
But for now let’s stick with the three-four month timeframe… The next consistent finding in the research is:
There’s a 3-4 month improvement window.
The bulk of improvement in pain takes place in the first 3-4 months after seeking treatment.
Pretty consistently7, any patient group with sciatica improves markedly for 3-4 months, then, on average, their pain scores plateau. This goes for both acute groups and mixed acute-chronic groups.
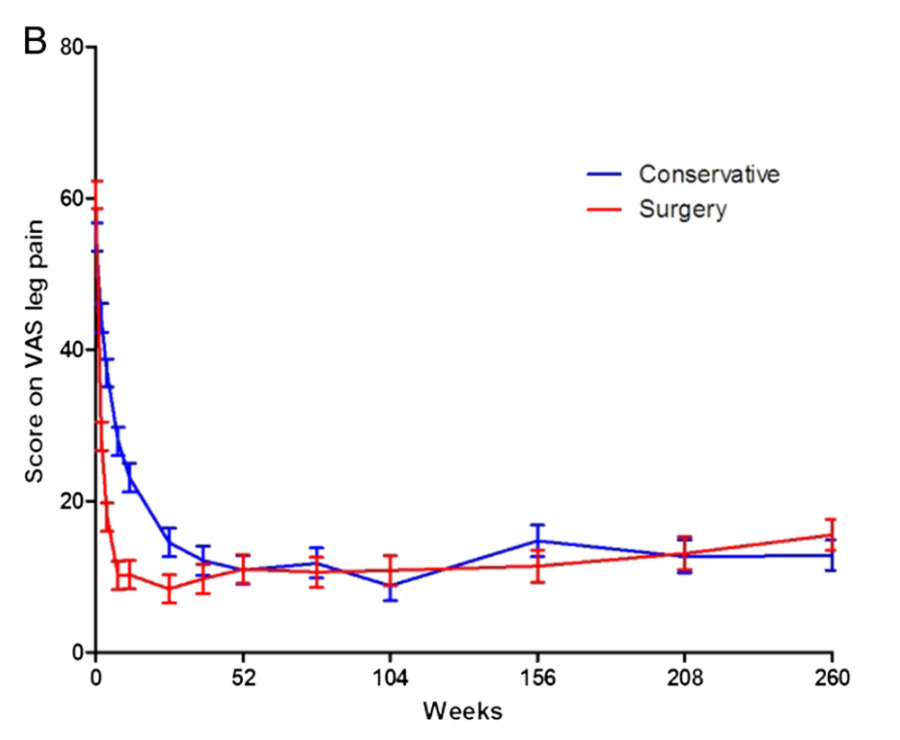
For example, Peul and colleagues found that mean leg pain scores levelled out in earnest at about four months of conservative treatment8.

The ATLAS study found that most improvement in pain took place in the first three to four months, then pretty much immediately levelled off. Patients in this study received a mixture of treatments, including surgery and injections for some.

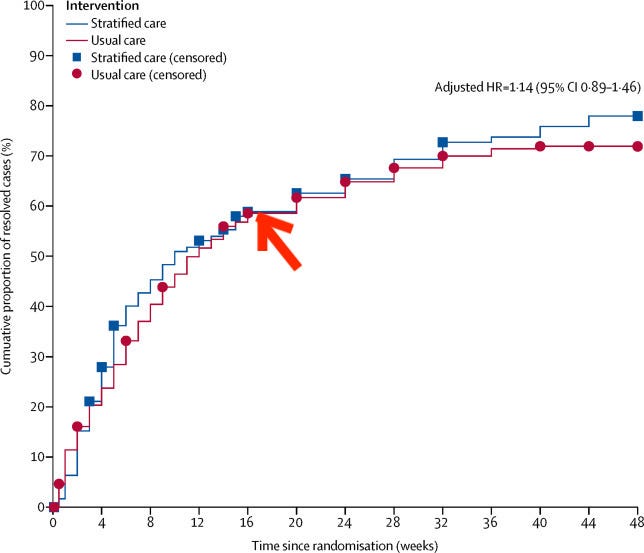
The SCOPIC trial observed a slowdown in 'first recovery from pain' rate at four months, with a definite plateau 7-8 months in.
There’s more. For example, the seminal Maine Lumbar Spine Study found that there was something of a plateau in improvement after three months, and a clear plateau after one year. Kim and colleagues saw a slowdown in improvement after three months, with a definite plateau at one year. Weinstein and colleagues - same story:

And beyond one year? The plateau keeps on plateauing on9: in their two-year follow-up, Peul and colleagues found there was no more improvement in the number of people saying they were happy with their outcome.

And after five years:
On the other hand, some studies do find slight group-level improvement beyond a year, over very long timeframes. Nykvisit and colleagues found little improvement between one year and five years, but a bit more between 5 years and 13 years. The Maine Lumbar Spine Study finds a slight improvement in outcomes between one year and ten years, but 45% of people in this particularly recalcitrant group (many claiming workers’ comp) still said they had not improved. And an old study by Söderberg found that over a decade there was very gradual group-level improvement:

And there’s no doubt that a minority of people with severe, persistent sciatica do suddenly get better, even after months and years of pain, and sometimes for no apparent reason. This was observed in the ATLAS cohort:

But it still looks like for most people, the bulk of improvement in sciatica takes place in the first three or four months after seeking care. After that, improvement on a group level plateaus, or at least nearly does.
Clinically, what it means is that we can encourage our patients to be optimistic for 3-4 months, but we should help them to be realistic beyond that. Certainly, past the 3-4 month window we shouldn't keep promising people that recovery is 'just around the corner’. Lots of people with sciatica get stuck with their life on hold.
“I think clinicians should be more honest from the beginning when they know there could be a chance of long-term pain. Mine weren’t.” - Patient advocate Tina Price, on her persistent sciatica.
Let’s continue. Mean group differences are one thing, but patients are probably more interested in their odds of being happy with the outcome. Luckily, we can estimate those…
4 out of 5 people happy after a year.
A year after seeking treatment, roughly 4 out of 5 people are happy with the outcome. Of the 1 in 5 with ongoing symptoms, perhaps half will say things have got worse.
4 out of 5 is a rough approximation of lots of studies.
For example, the SCOPIC study found that after one year, about 75% of people were completely recovered or much better. On the other hand, approximately 18% of patients said they were no better and 7% said they were worse10. Peul and colleagues found that although 95% of patients reported complete or nearly complete recovery at some point in the year of observation, by the end of the year this was only 82.5%, because some of those 95% recovered then relapsed. After five years there was no change.
There’s more: Weber and colleagues found that after one year, 70% of patients with acute lumbar radiculopathy were back at work and unimpeded in their leisure time. Another study by Weber and colleagues found that 80% of people had good or fair outcome. Hakelius and colleagues found that 4/5 of people did not develop long term pain. El Barzhoui and colleagues found a favourable outcome in 84% of patients. In their conservatively-treated group, Weinstein and colleagues found an 82.3% satisfaction rate.
In other words, a fairly consistent 75-85% “I’m pretty happy” rate at one year, which I’ve abstracted out as about 4 out of 5 people.
(Again it’s important to emphasise we are no longer in true natural history territory - many of these patients are receiving routine treatment, and have had pain for some time before the start of the study, so this is really the ‘clinical course’ of sciatica).
(Some studies find a worse than 4-out-of-5-are-happy rate, mostly because they deliberately recruit from a particularly chronic or severe patient group whom you would expect to do worse11. The exception that really bothers me though is the large, high-quality ATLAS study, which reported a measly 55% improvement rate by the end of the year, i.e, far short of 4 out of 5 people. Why? The study population isn’t that unusual, so I don’t think it’s that. Maybe the difference might have something to do with the measure of improvement they used, which was 30% or more on the Roland Morris Disability Questionnaire.)
So, if my estimate of ‘4 out of 5 people are happy with the outcome of care’ is wrong, it’s probably because it’s too optimistic… the true number might be less. Particularly for people with particularly severe or chronic pain.
Let’s continue on a pessimistic note and consider the important fact underlying all these numbers - once sciatica has gone, it doesn’t necessarily stay gone.
20-25% of people relapse.
When sciatica does resolve, there's about a 20-25% chance that it will come back in the next year, although it will not necessarily be as severe.
Suri and colleagues found that amongst 79 people who recovered from radicular pain and remained symptom free for at least a month, 25% had a recurrence in the first year. The pain wasn’t necessarily as bad as their initial attack. Half of these recurrences were in the first three months, and most of the rest were between 4 and 9 months, i.e. recurrences are weighted towards the first year or so. They also found that if people’s pain resolved quickly, it was less likely to recur.
The same team also performed an analysis of another trial, [EDIT - I originally linked to the wrong paper by the same authors here - if you are reading it now, link has been corrected] finding a very similar result: 23% of people who recovered had had a recurrence after one year12. They also found that if someone's pain had resolved completely - no niggling tension or anything - then recurrence risk was lower.
That’s about the best I could find for pure recurrence rates, but there’s a lot of data out there that confirms that the end of a sciatica story isn’t always, in fact, the end. For example, Peul and colleagues found that fully 23% of patients switched from being happy then unhappy with their outcome, or vice versa.

Söderberg found 40% of his cohort had some sort of recurrence that was bad enough to take time off work, whether a ‘pure’ recurrence or an acute-on-chronic one. Startlingly few people in his study were ‘one-and-done’ - just 14% got sciatica for the first time ever, got better, and never got it again. "Sciatica often runs a remittent course and serious recurrences can occur after years of freedom from symptoms", he writes.
Perhaps the best visual illustration of the twists and turns of a sciatica journey is from the analysis of the ATLAS trial by Ogollah and colleagues. Each green line represents one patient’s leg pain over the course of a year:

I think the lesson here is “this too might pass” - whether you’re recovered or still in pain, whether you’re having a good month or a bad month, there’s a reasonable chance you won’t stay that way.
Summary
In summary,
For people with very acute sciatica, there's a rule of thirds: Over the next couple of weeks, you have about a 1 in 3 chance of your pain greatly improving; a 1 in 3 chance of it improving a fair amount; and a 1 in 3 chance of it staying the same or getting worse.
For about half of people with sciatica, pain will resolve, or practically resolve, at some point in the three months after they seek care.
The bulk of improvement in pain takes place in the first 3-4 months after seeking treatment.
A year after seeking treatment, *roughly* 4 out of 5 people are happy with the outcome. Of the 1 in 5 with ongoing symptoms, perhaps half will say things have got worse.
When sciatica does resolve, there's about a 20-25% chance that it will come back in the next year, although it will not necessarily be as severe.
And 4-6 weeks? 4-6 schmeeks!
Okay, to be fair - the idea that ‘sciatica usually gets better in 4-6 weeks’ isn’t actually that far off, if you pick particular definitions of ‘usually’ and ‘better’! Most people really do feel better in the short term, many of them a lot better.
But the 4-6 weeks line is probably misleading, more often than not. It hides the fact that 1) about a third of people won’t feel any better in that time frame and 2) the two-thirds that do improve often have a few more weeks/months of niggling pain and recurrances, or worse.

A good alternative to ‘sciatica usually takes 4-6 weeks to get better’ might be ‘The worst pain is usually over in 4-6 weeks, but you’ll probably have some pain for longer. For the majority of people, this is manageable pain that eventually disappears within the year, but for a minority it’s more severe and persistent, or recurring.’ Not as pithy.
More eloquently, here’s the German surgeon Oppenheim, writing in the 1900s: “In many cases sciatica runs a favourable and rapid course and the patient makes a complete recovery within a few weeks or months. But in other cases the disease is fairly obstinate, it persists for one or several years, and then runs a fluctuating course, and even after healing there is a strong tendency to recurrence.”

The important caveats to everything above are:
Please think of the numbers in my conclusions as approximations, or rough summaries of trends in the research. They’re not really statistics per se.
People with sciatica that’s mild or short-lived enough that they never seek care aren’t included in these studies, so they aren’t represented by these conclusions. Similarly, people with sciatica that’s particulary severe, or who have lots of comorbities, are excluded from some of these studies, so they aren’t really represented either.
Most of these conclusions are drawn from - and therefore can only be apply to - mixed groups of patients with both acute, subacute and chronic pain, i.e. they are about the ‘clinical course’ of sciatica for your average patient seeking care rather than the true ‘natural history’ of sciatica. It’s safe to assume people with acute pain will have better odds and vice versa.
Probably if you’re going to tell your patients these numbers you should be clear they apply to population averages, and then perhaps make a guess at whether your patient come out on the better or worse end. A prognosis post is inthe works, but basically people with worse pain and more comorbidities, and people who’s pain is already becoming chronic, will probably do worse.
Most of all:
Thanks for reading - but please don’t just read! What am I missing? What have I said that doesn’t fit your clinical experience, or your reading of the evidence? Please comment on this post, or reply to the email. This is too important for you to let me get away with my mistakes :)
Til next time,
Tom
P.S. a few test readers of this post asked for everything in visuals/charts. I’m happy to do that but would rather wait for criticism + corrections to come in first.
The site does also say that even once someone is "much improved and virtually back to normal", they might have "low grade symptoms may sometimes persist for several months"
These conclusions are are not really data, but more like ‘rough summaries of the data’, or ‘the data simplified enough to be useful to you in advising your patient’. The aim is that they’re simplified enough to be useful, but hopfully not so much that they’re totally wrong.
Less recent onset than Vroomen but still relatively acute - viz, no longer than six months, with two-thirds of people having pain for three months or less.
Specifically, 76% of patients had a 'favourable' outcome at some point in the month after starting treatment, and 38% said they were free of symptoms. These numbers are slightly better than Vroomen’s, which can be partly accounted for by the longer timescale - a month instead of two weeks.
It’s also probably a lot of regression to the mean - i.e. people seek care when their pain is worse, and the only way is down.
That’s quicker than the SCOPIC trial and the trial by Peul and colleagues, which is probably because Hakelius and colleagues enrolled patients with very acute pain (in general, a more acute group is always going to improve more than a mixed acute/chronic group.)
There are some exceptions, for example Weber and colleagues found that mean leg pain scores levelled out after just one month, and Fjeld and colleagues found that in people with severe acute and subacute sciatica, there was no more improvement in pain after just six weeks.
Individuals still reached recovery throughout the year, but mean pain scores do not improve much - presumably partly because of people sliding back.
At this point I realised that this isn’t really a plateau as it doesn’t go *up* before levelling off… If you picked up on that, well done!
Exact results: 20% and 17% of people were completely recovered, 36% and 33% of people much better, 20% and 24% of people better; 17 and 19% of people no change; 7 and 7% worse.
For example, the Maine Lumbar Spine study found that after a year, only about 45% of people felt significantly better overall - much worse than 4 out of 5. This is probably because it deliberately recruited a fairly chronic group, lots of them receiving workers' comp. Similarly, Nykvist and colleagues reported that after a year, fully 81% of people still had sciatica, and 41% said it was unchanged or worse. In this case, the authors recruited people with particularly severe symptoms.
This increased to 41% at two years and 51% at three, but the authors say this is likely an over-estimate because of a methods issue.
Great post, definitely think these are a big step up from twitter comments! Great figure from the ATLAS study
Thank you for such a wonderful article! It would be great if you can share your opinion on the following points:
1. As you mentioned in the article, 1/3 of the people sciatica will have their symptoms stay the same or even worse after 4-6 weeks. Would you advise early surgery to patient if there is no improvement in 4-6 weeks? Or would you wait till 3-4 months of conservative treatment? ( Obviously, patient preference and other factors play a huge role, but lets just discuss it in a vacuum)
2. While I understand why you say that it is a clinical course but not a natural history of sciatica due to the research design, is the true natural history of Sciatica going to be really similar to what you shown here ? Given that physiotherapy effect on sciatica is quite modest according to your own narrative review.
Again thanks for such an awesome article!