
Herniation wars
Three camps assemble...

Thanks for subscribing to my newsletter on lumbar nerve root syndromes aka sciatica.
An earlier version of this post originally appeared in MSK Mag.
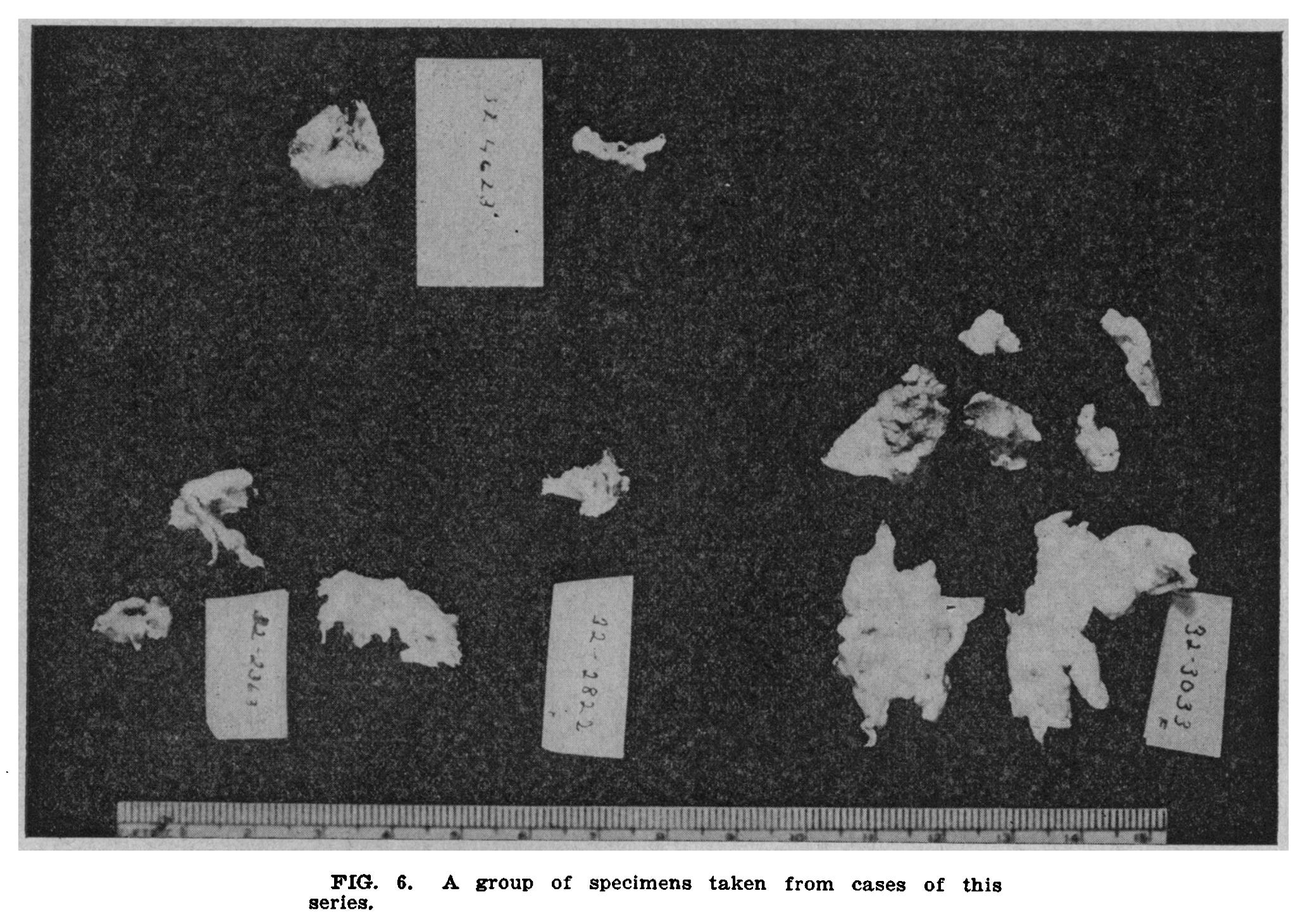
It all starts in the 1930s, in Massachusetts [1] [2]. A surgeon sees a patient who has developed acute sciatica after a skiing accident. The surgeon, William Mixter, operates on the skier's spine and removes a piece of whitish gunk. Mixter had removed this kind of material before, and he knows what it is: a benign tumour.
But then the skier's doctor gets involved. The doctor, Joseph Barr, says that Mixter’s benign tumour diagnosis doesn’t sound quite right. A tumour should cause insidious pain, but the skier's pain had started suddenly, after an accident.
They look more closely at the whitish gunk from the skier’s spine, and at a lot of other pieces of similar material that Mixter had kept from previous similar operations. And they realise that all these pieces of gunk are, as Barr guessed, not tumours at all. In fact, they're disc material. Disc material that has burst out from its home in the centre of the intervertebral disc.
Too Much Load
Mixter and Barr’s discovery sets the template for our early understanding of what causes disc herniations: that they’re the result of a trauma. In 1938, for example, one physician writes that "It is the opinion of most authors that abnormal protrusion of an intervertebral disk into the spinal canal is in the majority of cases the result of trauma" [3]1. By trauma, most physicians mean something sudden, but some also mean gradual trauma by repeated insults over time; the "slight shocks of normal life"[5].
Whether sudden or gradual, the earliest understanding of why discs herniate is essentially this: too much force goes through the disc, which makes it break. Let's call this school of thought the ‘Too Much Load Camp’.
It only takes a few years for many in the Too Much Load Camp to appreciate that only a minority of people with disc herniations actually report a trauma [6] [7]. As early as 1948, Falconer writes that trauma has been “overemphasised” [5]. Another physician notes that "70-80% of patients give no history of injury. It is reasonable to assume that injury is never the sole causative agent and, when evident, is only an additional factor" [8].
Unhealthy Disc
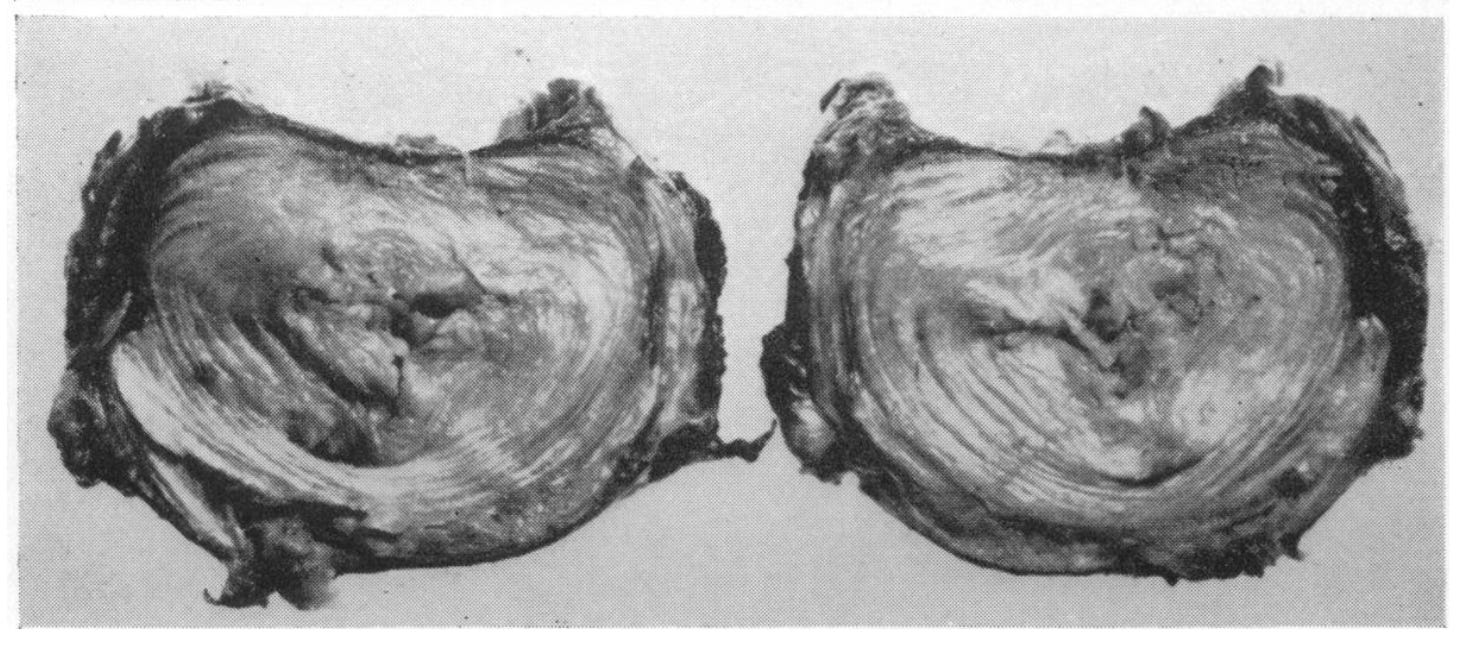
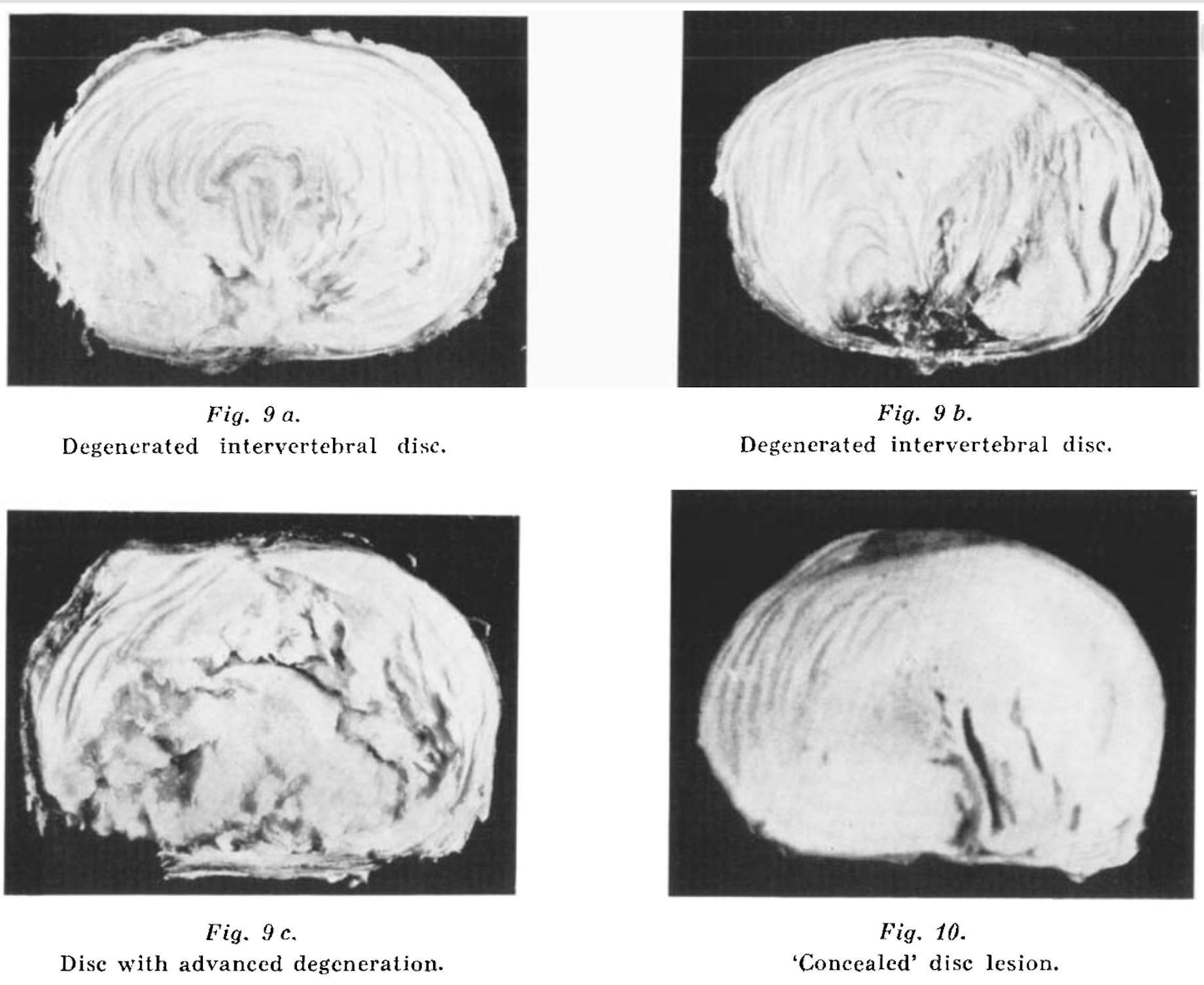
Where do mid-century physicians go when they leave the Too Much Load Camp? Well, they had long observed that while some discs stay plump, white and healthy, very early in life some others become thinned, yellow and fissured. And they see that these particularly unhealthy discs have slipped into a nasty state of imbalance between catabolic and anabolic activity. They label them as degenerated [8][9].
If it’s not trauma that makes discs herniate, they hypothesise, then it must be this degeneration. “There are other more important basic factors [than trauma]”, writes Naylor in 1962, “herniations most probably develop as a result of a more general collagen/polysaccharide disorder”. In other words, it’s not the load placed on the disc, but the qualities of the disc itself that cause it to weaken and fail. Let’s call this new school of thought the ‘Unhealthy Disc Camp’.
So if the Unhealthy Disc Camp says that degeneration causes herniations, then what causes degeneration?
It’s partly, they say, systemic health. If you smoke, drink, have diabetes or vascular diseases, sleep poorly, work more than you rest and so on, then your discs have an even harder time maintaining themselves [10–13]. Smoking, for example, reduces the metabolic activity in your discs and weakens their structure [14–16].
And it’s partly just that discs are particularly vulnerable to degenerating because they are avascular [11]2.
All In The Genes
Let’s fast forward to the nineties. Researchers have long suspected that disc degeneration is hereditary [8], and a group in Finland decides to find out. They recruit lots of sets of twins with different exposures to the usual risk factors for disc herniations [17]. For example, maybe one twin is a farmer and the other is a reporter; or one is a smoker and the other isn't. Then they put all the sets of twins in MRI machines to look at their discs. And they see that lifestyle factors have barely influenced those twins' discs at all.
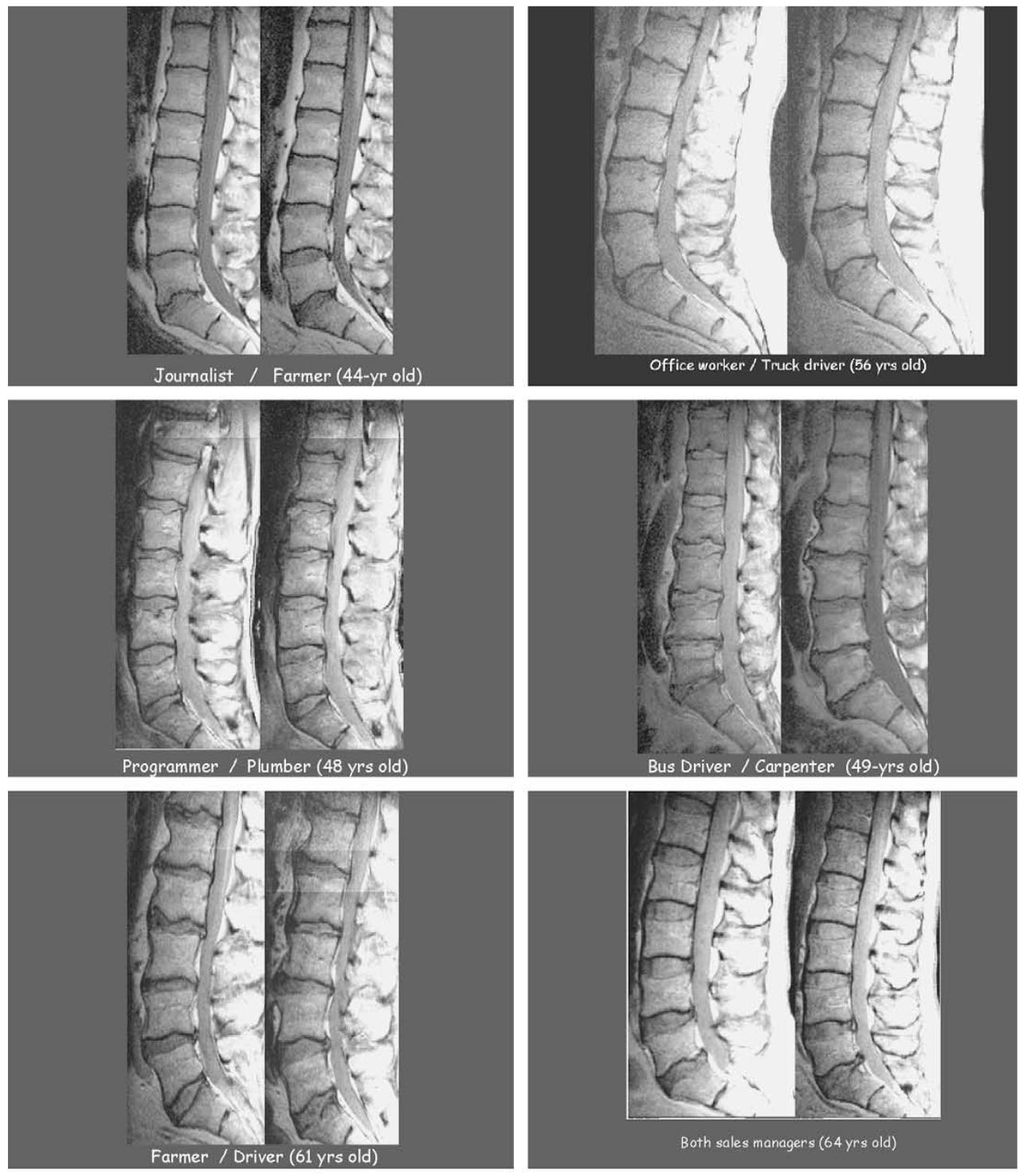
With the Twin Spine Studies, what we can call ‘All In The Genes Camp’ is formed. “61% of the variance in disc degeneration is explained by familial aggregation”, the authors write a few years later, summarising their findings. “Disc degeneration, which was once viewed as a result of ageing and ‘wear and tear’ from mechanical insults and injuries is now viewed as being determined in great part by genetic influences" [17].
How does your genetic makeup make you more likely to have a disc herniation? People in the All In The Genes camp don’t claim that there's one gene for disc herniations, but that you might be predisposed by a complex interplay of multiple genes [18] [19]. Those multiple genes might, for example, conspire to make your discs’ collagen matrix weaker, or make the enzymes in your discs more active. That means that ultimately, as you get older, your discs are going to do what they’re going to do - whatever your occupation or smoking status.
But it’s easy - and common - to overstate genetic influence on disc herniations.
For one thing, the estimate of familial influence on disc degeneration in the lower lumbar discs, i.e. the ones that herniate the most often, was just 32% [17]. That’s hardly a slam dunk for the All In The Genes.3
To be clear, the Twin Spine Studies’ estimate of occupation and lifestyle factors is much, much smaller than its estimate of familial influence. So genetics is clearly extremely important. But the studies’ biggest category of influence on lower lumbar disc health wasn’t, in fact, familial influence. It was just labelled… ‘Unexplained’!
Could there be something here for the Too Much Load camp?
Too Much Load Revisited
True, the evidence suggests that occupational and recreational loading has only a modest (but non-zero) effect on disc herniations [25–28]. But research into occupational and recreational exposure can’t account for brief, one-off spikes of excess load: a weekend spent moving house, for example, or a slip on the ice… And some researchers argue that it’s just these spikes of excess load - injuries, essentially - that are pivotal in the life course of a disc, and can set it on the long path of structural failure and eventual herniation [29–31].
And Too Much Load theory does explain something that genetics cannot: why so many people have just one or two herniated discs, while the rest of their spine is fine; and why those herniated discs are frequently the lower lumbar ones, i.e. the ones that work the hardest [32–34]. As Adams and Dolan argue, the most parsimonious explanation for this is discrete trauma [30].
This all flies in the face of the prevailing optimism, in some quarters, that discs adapt well to load and heal from injuries. And it’s true of course that discs adapt; it would be strange if they didn’t [35]. But they don’t do it that well. The best evidence that discs get healthier with exercise is all in recreational runners [36–38], but recreational running is the exact type of predictable, moderate load that lab studies tell us their discs should love [39], and therefore adaptation to running is hardly good evidence of discs’ anabolic power more generally4.
And when it comes to healing from injury, well, they definitely can’t do that. “Adult discs are incapable of repairing gross defects”, write Adams and Roughley [30]5.
Tyre-d of fighting
Joseph Barr, the doctor we met earlier, the one who started all this trouble back in the 1930s, never threw his lot in with any of the three camps. In 1951 he explained his position by likening disc herniations to a car tyre failure:
“The tyre, when it leaves the factory, may have a defect in the fabric (congenital weakness) so that it blows out while rolling along a smooth road. A tyre may blow out when it strikes a stone or curb (acute trauma), or it may give way thousands of miles later. A tyre exposed to gasoline ages rapidly, and degenerative change produces early tyre failure [42]".
Genetics, or ‘congenital weakness’ as he calls it, turned out to be far more important than Barr expected; but his analogy still holds. It captures well that while the various causes of disc herniations are interrelated, each one might predominate in different cases. Back to the patient’s story.
Reference list: click here
More detail on lifting, bending & disc herniations: click here.
Thanks to Felicity Thow for help with editing this piece.
And another, Eck, in 1942: "trauma is the precipitating factor in most cases" [4]
That means that they have to acquire most of their nutrients and expel all of their waste products using diffusion, which is a remarkably inefficient way for such a large, highly-loaded tissue to maintain itself.
Not to mention, the Twin Spine Studies studied disc degeneration, not herniation, and they’re not the same thing. Not only that, but there are also some technical issues that make twin studies, especially older twin studies, liable to overestimate heritability see [20] [21].
On the contrary, the laboratory evidence - and in fact some of those studies in runners - still tells us that higher-magnitude load is probably catabolic for discs [38] [39]. In any case, the runners-have-healthier-discs studies don't actually tell us that the discs are healthier because of the running. After all, compared to non-exercisers runners surely have many other healthy habits and genetic advantages that might make for healthier discs. In fact, an RCT found that a running intervention did not make discs healthier (or unhealthier) [40].
And “It is clear that an already damaged or degenerate IVD is unlikely to respond to loading in the same way that a healthy IVD does”, say Belavý and colleagues [41].
Thanks Tom. Good article. You have covered the history nicely. Do you notice that much of the problem is the propensity of scientists and clinicians to seek the ONE cause of clinical presentations. Clinical presentations are just groupings of like cases. We know that acute sciatica may be "caused" by a number of different factors that may or may not partially contrubute to the pathology resulting in the presentations, but still there is this apparent desire to find the ONE cause. Is that because they want to promote their own preferred treatment? Anyway, keep up the good work
As Tom says above it's human nature to want a cause and often patients seek this when they present to you. We often associate knowing the cause will lead to knowing the solution. The art then is the physio-patient relationship and communication of all of the above without trying to overwhelm and provide tangible take aways. How complex and fun.