Thanks for reading the 23rd edition of my sciatica newsletter. This newsletter tracks my research as I write a book about lumbar radicular pain!
The first sunrise of the year, this morning. At Galveston, TX.
Happy new year!
Let’s look back at the first year of the sciatica newsletter.
One year ago I wrote this tweet:
Over the next couple of months, I slowly got going with the project and tried to think of what it might look like.
But I soon realised you can't do things like this behind closed doors. Learning is social! You need other people to encourage you, give you feedback and point you in new directions.
I decided an email newsletter was the best way to do this. I can't honestly remember where I got the idea. I don't think I subscribed to any other newsletters I was copying. I think I had just heard of substack and thought it looked cool. I sent this tweet:
200 people signed up straight away, which was a nice boost! Since then, this newsletter’s subscriber count has been a slow and steady upward line, interrupted by sudden jumps if a particular post goes mini-viral or is shared by a physio #influencer. There are now 1,572 subscribers.
Starting this newsletter was one of the best things I have done for my professional and intellectual life. There's nothing quite like knowing an email will go out to hundreds of people to make you make sure you get it right. I think its spurred me to do high quality work. I get replies regularly, sometimes just a line or two, sometimes much more, and I enjoy and appreciate every one of them.
My first email started out like this:
Where am I going with this??
I want to create a really, really high quality source of information on radicular pain, for patients and clinicians. Yes, that’s very vague. I don't know what format the finished product will take. Whether it is a website or an ebook or an online course… Not sure.
Somewhere along the line I realised I was writing a book. It just seemed like the best way to communicate what I want to say and the best way to communicate with lots of people.
The first newsletter also contained these bits of personal news:
Personal news! After many months of waiting I finally have my interview date for a green card! We have an appointment in Detroit in April to prove our marriage is not a hollow sham.
More personal news! We also found out last week that in the summer we are moving to Houston, Texas! The "found out" part is because my wife applied for postdocs in a few different places and we weren't sure where she would "match". Very excited. 🤠🤠
Because of the virus, only the second one of these things actually happened and we are still patiently waiting for the first.
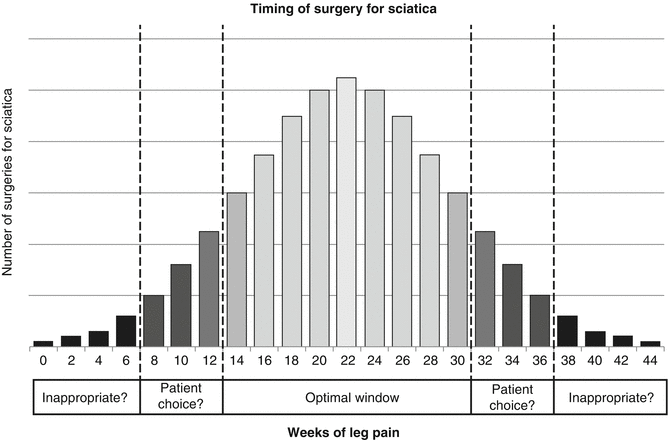
In the second email, I summarised the literature on the timing of surgery for sciatica.
So, the pro-surgery spin on this would be "early surgery saves a lot of suffering and if you wait, lots of people still end up getting surgery." The anti-surgery spin would be "if you wait, you can save 60% of people from surgery and although they suffer more in the short term it doesn't make a difference in the long term." Peul speaks very well on this.
When it comes to answering our question on the timing of surgery for sciatica, I think this study says it’s okay to wait, but don’t wait too long. I found the following picture on google images, made by Peul. I think it is a great visual summary of everything I have written above:
The position of the roots relative to the disc is important. As you can see here, the roots are actually kind of out the way of the disc when they exit through the foramen (and even so, far lateral disc bulges are relatively rare). The roots are most vulnerable to a disc herniation is just as they exit the dural sac. So if you imagine a paracentral L4/L5 disc bulge in this picture, the transiting L5 nerve would be affected.
I started the podcast in June. David Butler was the first person I emailed to ask to be a guest. I actually emailed the generic noi-group email address and he emailed back from his personal address, I think within a day or two. I was completely thrilled. I wasn’t sure how to approach the interview though. David is so prolific in his writing, and so generous in sharing his knowledge over the years, that I struggled to think of topics to cover that he has not already covered elsewhere. In the end, I abandoned any idea of making it a proper "interview" and just tried to have the conversation I would have with David if we were sitting in the pub with a pint.
Tom Jesson: You said in that book [The Sensitive Nervous System], a line that stuck with me because I think it’s one of the reasons I’m particularly interested in radicular pain. it’s that radicular pain is a particularly frightening thing for therapists to be encountered with.
David Butler: Yeah, that’s a really important thing. And that probably also leads into a lot of my more recent work, which, if I can express it like this, you can talk or provide a context for a patient that takes some of the sensitivity out of the system. So whereas in the old days I might have gone in, and let’s wriggle this, let’s move this, let’s pull this, [now] I’ll sit down and see what other things are going on so we can… take the sensitivity out of the system. And with our knowledge of how quickly that can happen, whether that’s neuro chemistry changes or even ion channel changes. Perhaps the education paths become important…
It was after I interviewed David that we made the long trip West to visit family before driving back East again to settle in Houston. Although this was a trip we made by necessity, it was also not too far off a dream holiday for me. I can't believe how lucky I am to have seen half a continent like this.
I started writing and recording more consistently over the summer. I was really pleased that I contacted Daniel Albrecht to talk about neuroinflammation, and doubly pleased that he was such a good interviewee. I think this interview is one of the most high-value things I did with the newsletter because it built another little bridge between clinical practice and basic science research. In the next year, I hope to do more of this (although, forgive me for saying this, many academics I have emailed simply do not reply, even to follow-ups. But all the more reason for us to appreciate those who do, like Giacomo Carta).
The first thing to say about neuroinflammation is that it is not in itself pathological. Just like inflammation in the muscles, joints and skin, inflammation in the nerves arises in response to dangerous stuff like pathogens or tissue damage. Many different cells and molecules work together to limit the danger and repair any harm done. Neuroinflammation only becomes a clinical problem when there is too much of it, or it goes on too long.
The second thing to say is that it is not really something that is turned "on" or "off". We use words like "activated" to describe microglia, which makes this confusing. But really it's a "more" or "less" process, not "on" or "off".
At one end of the continuum, transient, low level immune signalling is involved in the normal development of memory and learning and arguably doesn’t qualify as “neuroinflammation” at all. At the other end "very rapid and dramatic" neuroinflammation kicks in after serious nerve injuries.
I was also pleased that I spoke to two people with sciatica on the podcast, Kate Charlton and Drew Jordan. Part two with Kate is coming in the new year.
At the end of every newsletter, if I remember to, I ask for feedback, especially if people disagree. I get lots of feedback, but almost none of it is disagreement. It’s not because I'm right all the time, but because even when I invite disagreement people are too polite to provide it. So the only newsletter I got any pushback on was the one where I tentatively endorsed gabapentonoids, in very specific circumstances.
On reading that these large, high quality studies found no benefit, my first question was: Did they select patients with *neuropathic* radicular pain? After all, radicular pain is a very mixed bag of nociceptive, inflammatory and 'nociplastic' mechanisms, to name just a few. But I would only expect gabapentin to be effective for the subgroup of people with neuropathic pain, meaning actually damaged, not just irritated, nerves. People with severe shooting pain, numbness, pins and needles, etc. If the trials jumbled up these people with all the other mechanisms of back and leg pain, then no wonder their results are negative.
In August I asked for people's questions about sciatica. I didn't have time to write a proper newsletter because we were on the road, travelling east from California to settle for the next two years in Houston, Texas.
As for those questions, I have replied to some of them in newsletters, some I asked in podcasts, and some are still unanswered in a file that I have not forgotten about, I promise! One reader asked how long loss of nerve function takes to recover after radiculopathy. The research was patchy but I reached the following conclusion:
So, it seems that
Loss of function recovers most quickly in the first three months or so
Even after a year or more, people can still recover function
Sensation might take a bit longer to return than strength
At least 10% of people and maybe as many as 60% will not regain full function.
The most popular newsletter in terms of page views was my interview with Annina Schmid. I owe Annina a lot. I met her at a conference I think two years ago. I was amazed at the time that she was happy to sit and chat with me about antidromic impulses and axonal reflexes. When I was leaving England for the States I knew I would have a period of time where I would be unemployed, so I wanted to take the opportunity to do some research. I contacted Annina with some ideas, which she politely told me weren't very good. But she suggested a better idea and, along with my friend Nils, we worked together on it over the next year or so and it became my first peer-reviewed publication this summer. It's no surprise to me the newsletter with Annina’s interview has been the most popular.
As I research radicular pain I find that it is continually, fractally interesting. Each new cool thing leads to another cool thing. Devor's theory of the dorsal root ganglion, which I wrote up in the 16th edition of the newsletter, is just one example.
Apparently there are very few parts of the nervous system that are outside the blood-nerve barrier. One is the part of your brainstem that elicits a vomit reflex, called the chemoreceptor trigger zone. It can detect instantly when noxious substances are in the blood stream and trigger a protective mechanism: puking.
Devor argues that the DRG has a similar role. For example, if you are sick it can react to circulating cytokines in your blood stream and trigger the aching limbs that make you want to rest and recuperate.
This theory also helps explain why the DRG is able to generate its own action potentials. Although its jumpiness contributes to the misery of many people with radicular pain, it is part of an evolutionary trade-off: we gain a chemoreceptor and in return accept a greater susceptibility to painful neuropathies.
If Devor's theory is true, maybe we can think of the DRG as being like a scout sent out from an army's camp to surveil the area: although it’s vulnerable, it can gather important information…
The interior of the human intervertebral disc is cut off from the "outside world" of the rest of the body. Except for the outer few millimeters, the disc has no nerve supply and no blood supply. Nerves and blood vessels cannot infiltrate through the tightly bound, high-pressure fortress of the annulus and the cartilaginous end plates. And for added protection, this fortress is patrolled by cell-destroying molecules.
If the annulus cracks or the disc herniates, the fortress maintaining this immune privilege is breached. This is the first time in a person's lifetime that their disc material is presented to their immune cells. Those immune cells (T cells), unable to differentiate this foreign substance from a pathogen or toxin, initiate an inflammatory reaction, recruiting other immune cells (lymphocytes, macrophages) to the area.
(That edition also contained my favourite pun of the year, “disc-ow inferno”.)
I have had to take a break from the podcast in the last couple of months. Producing and editing it is surprisingly time consuming. Especially as I try to read as much of a guest's publications as I can before speaking to them. I will re-start the podcast after I finish my book when I feel under less time pressure. But the last two podcasts were great. One with Mark Laslett, the other with Raymond Ostelo.
The most recent two editions of the newsletter, on dermatomes and piriformis syndrome, have been two of the most popular. Partly because they are both of obvious immediate clinical relevance. But also because, for whatever reason, people just love finding out that stuff is wrong! I first learned this when I wrote about myths and misconceptions in physio three years ago (I'm now a bit embarrassed about how sure of itself that blog post is, but it still holds up mostly).
It has been a pretty bad year in many ways, which I won’t go into. But this newsletter and the work it covers have been an unmitigated good thing for me. I am really grateful to everyone for reading it, sharing it, and replying to it.
Let's end the year in review by looking forward to 2021. As I mentioned in a recent email, I am going to put out by book in two parts. The first part will be in February. I don't want to try to guess how long the second part will take, but it should be done by the summer.
After that, I don't think I will keep this newsletter as a radicular pain newsletter. I might change it to a general research review. I like summarising papers and putting them in context. I also like the idea of reviewing a "classic" paper every week instead, since, let's be honest, there isn't really practice-changing research released every month, never mind every week! Finally, I am also thinking about researching red flags and identifying serious pathology next. So the newsletter could be about that. I think it is the area where I can make the most impact with my writing. Although it might seem obvious to say, by getting better at identifying serious pathology earlier worldwide, we can reduce human suffering. Considering how much more I am writing about this idea than the other two, I think it might be the one closest to my heart.
I'll leave it there for this week, and for this year! If you have made it this far, thanks for indulging me in looking back on this newsletter and its role in my life over the last year. Normal service will resume next week!











great summation Tom. Have a good year...